With a unique perspective shaped by my own learning disabilities, including ADHD, I bring a wealth of professional expertise in education and health policy, grant review, as well as research, evaluation, and treatment of children with speech, language, and reading disorders.
My passion lies in advocating for those who are not able to do so for themselves, leveraging my diverse background – both personally and professionally – to make a meaningful impact in the field of special education and child development.
Stephanie M. Nixon, Ph.D., CCC-SLP January 29, 2025
The power of a name, label, or diagnosis – even the name of a symptom
What’s in a name? A label? A diagnosis? Does knowing a diagnosis grant us power? Does it provide the knowledge we desire when confronting a situation (not just learning disability or health-related)?
When I wrote about this years ago in my undergraduate thesis about Egyptian religion, I noted the similarity between naming gods and goddesses who “controlled” various aspects of life (love, weather, sun, rain, etc.) and naming hurricanes. I know this is over simplified in some ways, but there is a parallel.
“Sometimes naming a thing — giving it a name or discovering its name — helps one begin to understand it. Knowing the name of a thing and knowing what that thing is for gives me even more of a handle on it.” — Octavia E. Butler, Parable of the Sower
Thinking about what Octavia E. Butler said above, it makes sense (at least to me). It helps to just understand sometimes. And other times, it might bring a “fix”. Granted a often there isn’t a “fix” or “cure” for learning disabilities or chronic illnesses or even natural disasters. i.e., It’s not always just here, take this medication for 10 days and you’re all better. (I wish it was that easy…)
For ADHD and autism, there are no cures but there are treatments and there is understanding.
For chronic illnesses like my diagnosis of Hashimoto Thyroiditis, often there is no cure. You might need to take a medication daily depending on your doctor’s advice. Some chronic illnesses are even progressive. Some are merely described via symptoms, but we cannot “cure” it.
For natural disasters, we cannot stop the hurricane from hitting an area, but we can prepare for it. And we can provide disaster relief afterwards to help an area recover
What have I seen, personally and professionally?
As a practitioner, I sometimes patients/caregivers wanted a diagnosis and others wanted the descriptor and support. For adult and pediatric patients, a label can help with insurance coverage. For pediatric patients, a label (i.e., a diagnosis – even working diagnosis, e.g., autism, dyslexia, etc.) can help with access to special education services and accommodations and insurance coverage for services.
As a patient, adding the diagnosis of autism to my long-time diagnosis of ADHD helped me understand those feelings of overwhelm from too much noise, too many “things” coming at me, and much more. Has it “fixed” the situation? No. But it gives me grace in those moments or even afterwards when I can recognize the link to “autism”. (I recognize this won’t apply to everyone. Some people find hearing the actual diagnosis scary.)
What’s in a name?
When it comes to chronic illnesses (even acute), speech and language disorders, learning disabilities, autism, ADHD, and more, we as patients (and even practitioners) often want to know the diagnosis/name. We want to understand what we’re dealing with. But why?
Empowerment, knowing how to prepare, find options, and find ways to cope (social groups, etc.)
Validation, knowing what we feel/see is happening, someone else sees it
Understanding, understanding of ourselves and what we need and for parents of a child, understanding of a child’s needs
Forgiveness of ourselves (our children and loved ones where applicable), knowing a “diagnosis” can help a person recognize how the diagnosis affected a situation and forgive themselves or another for this. (I’m not saying a diagnosis is an excuse! I’m saying, it can give that allowance to make that mistake.)
Access, having a diagnosis or adequate symptom description can give access to accommodations, insurance coverage, and research studies that are otherwise unavailable. (e.g., For pediatric speech-language therapy, many private insurance plans have exclusions saying that services are only covered in cases of accident, injury, stroke, or autism spectrum disorder.)
What do many patients want?
As a patient, I want to be heard. I want to be validated. I am living this life, not the practitioner. I want that practitioner to treat me like I treated my patients, which is to listen, genuinely listen. Don’t discount what I’m telling you because you aren’t seeing it in this moment at this time.
When I saw patients, I tried to remember, treat them like I wanted to be treated. Yes, they may want the why, the cure, the fix, but I did my best to explain what I saw and next steps. And hear their responses and consider them in light of what I saw in that 2 hours in my office.
And of course there are times we may find nothing definite, but we can validate their experience. We can listen. We can recognize when there is something off that just may not be recognized by available tests.
There are many times that there isn’t an exact diagnosis. We can describe the symptoms and those might even have “diagnosis codes” in ICD-10, but we may never know the overarching “cause” for those symptoms or if there is one. BUT, even describing the symptoms and assigning ICD-10 codes provide a “name”.
Like many of my families and patients I have had over the years, I have navigated the waters of the unknown with my health and learning. I know how scary those waters can be. I know there isn’t always an answer, but my objective is to benefit others with my knowledge and experience. Even if it’s just how to navigate healthcare systems or health insurance or a diagnosis/symptom.
More recently, I decided to record some of my symptoms and post them to YouTube to share the journey with others. My hope is that professors, practitioners, and patients can benefit from these in some way.
Would I like to know a cause? A name? A diagnosis? Who wouldn’t? BUT – even if I can’t learn that information – if I can benefit others, then in my opinion I won.
Thoughts for providers
Providers, if you are frustrated by patients seeming “hung up” on getting that “label”, it’s for the reasons I said above. What can you do?
Respect the request – and try to understand
Sit in their shoes a minute
Ask the patient/family why they seem to “want” the diagnosis
Consider whether they experience something you may not see in your office
Use your active listening skills
Consider reviewing the data and scheduling a follow-up
Avoid assuming you know more about that patient than the patient/family (you only see them for that short period in your office)
Empower them to help you see what they see
Ask if there is an insurance reason they need a diagnosis
Consider whether the person could benefit at minimum from an acting diagnosis (if appropriate) to give them access to care that would otherwise be denied
Ask them how what they report is different than previous function (if appropriate)
Ask how it is affecting them in daily life
Tangent. Consider a patient’s background during the appointment
If that patient is an allied health professional trained in the area they are coming to you about, please pause and consider that this patient may be using every tool they know to minimize the effect of their concern in your office. Listen. Think about the tools they might have – objective tools (like a measure of grip strength for OTs) – that you don’t.
An example from many years ago
Over 10 months from 2010 and 2011, I went through over 20 rounds of antibiotics for respiratory infections before seeking a pulmonary doctor. Finally, I went in. My voice was hoarse from all the coughing. I told the doctor (who will remain nameless) that I was going to lose my voice. I asked for someway to help the cough so I wouldn’t lose my voice. (Try being an SLP with no voice.)
The doctor told me I wouldn’t lose my voice. I reminded her of my training. I reminded her of my specialty. I was dismissed. I was in tears trying to explain myself to her.
Fast-forward. The sputum culture returned. It was Methicillin Sensitive Staphylococcus Aureus. I was given an antibiotic. But due to coughing, I lost my voice 24 hours later. I did not regain enough voice to return to work for at least 3 weeks. (Even when I returned, I barely had enough voice to talk through the day.)
I saw an ENT who specialized in voice, who said I had an ulceration on my vocal folds from coughing.
To patients and practitioners
I understand the frustration from both sides. I’ve been there. I’m there right now. I know how scary the unknown is, but let’s work together. Let’s listen.
Practitioners, involve patients who want to understand when reviewing their case. Don’t hesitate to say “I don’t know” or “I need to go look that up”. Just be sure to get back to the patient later.
Patients/families, I know the information is sometimes overwhelming. Don’t hesitate to pause the practitioner, repeat what they said, and as if you understood. As for a list of action items. And tell the practitioner if you have any barriers to accomplishing those items (even time to make those phone calls). Find out how to contact your practitioner. You deserve someone who will listen and advocate for you.
So…again, what’s in a name, a label, a diagnosis? It can be more than a provider might know from access to understanding. Validating a symptom observed goes a long way, especially if that has an ICD-10 code – even if there is not treatment available. And that ICD-10 code is something researchers might look up in the system in the future and look at associated health conditions which could lead to better understanding and treatments.
Yes, that might be a long way off, but again, for someone like me who just wants to help others, I don’t care if it’s 100 years off. If my data helps practitioners and patients learn about health conditions, then I will view it as a win.
Disclaimer. This article is based on personal and professional experience as well as research on counseling patients. This information is not intended as legal advice or healthcare advice. Please see a provider about any healthcare needs. I acknowledge that some people need different approaches than others when receiving information, so again, providers use your informed clinical training and judgment.
A medical claim is a bill that your provider sends to your health insurer for your medical care (or if “out-of-network”, a claim you send to your health insurer). (This claim includes codes called CPT codes – or procedure codes – associated with the costs.)
A prior authorization (also called precertification) is when your health plan requires patients to get approval for a medical service or medication before they receive the care. Information from your chart must be submitted from your chart by your practitioner (and sometimes by you). (I will address PAs more in a later post.)
When I refer to denial in this post, it means denial of a code on a medical bill or denial of a prior authorization request.
But remember there is a difference. And you can sometimes prevent medical claim denial by confirming whether precertification or prior authorization is needed for a medical service.
For a medical claim, the medical service was already completed and the bill was filed with insurance. You could be stuck with the balance when there is a denial.
For a prior authorization, the provider is requesting that your health insurance company agree to pay for a medical service. The service has not been completed.
Note. As an SLP, a frequent reason that I saw claim denials and prior authorization denials by private health insurance companies for a child’s speech-language therapy services was the plan did not include “habilitative” services OR only included them for autism spectrum disorder. i.e., “This service is only covered in cases of accident, injury, stroke, or autism spectrum disorder”.
What I do. I often call to confirm coverage of any services I am going to receive (or when I was providing services to patients. I ask these questions: Are there any exclusions?Do I need prior authorization? If the answer is yes to either or both, I ask for additional information about these. I take notes. I write down the date, time, and name of the person on the phone. I put that information where I won’t lose it. (Take a picture, put it in the notes app on your phone, anything.)
What is downcoding during claims processing?
The health insurance company changes a higher-level CPT (i.e., procedure) code (e.g., CPT 99214 indicating moderate complexity over 30 minutes) to a lower-level CPT code (e.g., 99213 indicating low complexity 20 minutes).
No matter in- or out-of-network it results in lower reimbursement as the lower code is associated with a lower payment amount.
An example from one of my out-of-network claims where my health insurance company used downcoding for a CPT code.
Column A = Billed Amount Column B = Member Rate (nothing there because this is out-of-network) Column C = Not payable by plan Column D = Applied to deductible (I hit my out-of-network deductible early this year.) Column E = My copay (does not apply to out-of-network) Column F = Remaining amount (Amount billed – Notpayable) Column G = Plan’s share (For me, this was 75% of the amount they deemed appropriate after downcoding) Column H = My coinsurance (For me, this was 25% of the amount they deemed appropriate after downcoding) Column I = My total share (Coinsurance + Not payable by plan)
You (and your practitioner if they are in-network) must watch your explanation of benefits for downcoding. This isn’t something they will tell you with a phone call or an email. It appears with those numbers referencing the reason which is at the bottom of the bill.
So if you see those numbers, look for a reason. If you are struggling to read the explanation of benefits, then ask a biller at your hospital, the specialist, or you could even email me.
Health insurance companies will say they do this to prevent upcoding by practitioners (which is fraud).
What do I do now?
Review the denial notification (These are not easy to understand for anyone – even some doctors can’t read an Explanation of Benefits. Ask for help from your provider, insurance company, a friend, me, anyone, if it’s confusing)
Contact your provider
Contact your insurance company.
Ask them why
Ask what can be done to correct the claim
Sometimes it is a simple processing error. (Once my annual woman’s exam was processed by my health insurance as if my husband was the patient, despite this clearly being inaccurate. It was reprocessed correctly without an appeal)
Other times the doctor didn’t provide enough information, or the insurance company needs to see case notes.
Gather the documents you need (medical records, test results, practitioner notes)
File the internal appeal: This information is on the explanation of benefits, and sometimes you can do this through your health insurance online portal.
If you need to fax the appeal, then keep a copy of the sent receipt. (I use e-fax.)
If you need to snail mail the appeal, then note the date and time you sent it or even send it certified mail return receipt. (I say this after having my private insurance claiming they did not receive documents multiple times.)
Learn about the appeal process:
DEADLINES are important (set calendar reminders, whatever you need to follow-up on these)
Know what to do next if the appeal is denied: Sometimes you file an external appeal, sometimes you have another level of internal appeal
If you are struggling with the process, then contact your State’s Insurance Department (often there is a regulatory body like an insurance bureau and a group that helps navigate appeals)
Less than half of the 45% who reported the errors challenged the errors. Why? The most reported reason said they didn’t know they had the right to challenge a medical bill.
About 2 of 5 who challenged (i.e., appealed) their bill, reported it was reduced or eliminated by the insurance company.
17% reported that their insurer denied coverage for care recommended by their doctor; more than half said neither they nor their doctor challenged the denial
About 6 of 10 adults who experienced a coverage denial also experienced delayed care
There are many issues cited in this report including how complexity of US health insurance has affected patients. These patients may struggle to understand what is and what isn’t covered and their financial liabilities.
Personally, even selecting a health plan each year is complicated by terms like the following:
HMO
PPO (but some of these are really HMOs pretending to be PPOs)
Wait! There’s more! Then you have 105% of the maximum allowed medicare rate for out-of-network
Then how much of the out-of-network bills go toward your deductibles? Does all that go toward the max out of pocket out-of-network? (You’d be surprised.)
Does the coverage change based on the service? (Yes.)
Do they change coverage based on the service provider? (i.e., facility vs. clinic)
Are there a maximum visits?
With my insurance cover allied health services (i.e., speech-language pathology, physical therapy, and occupational therapy)? How many visits per year? Are these capped individually or across services? Copay? Are there exclusions?
The list goes on…
What can I do if I lose the appeal at all the levels available?
If your plan is through your (or your spouse’s) employer: Explain the issue to HR at your company. There might be something in what they negotiated that could change the situation, or they could negotiated better benefits for the next plan year. Some employers even have support available for employees in these instances.
Advocate. You could also contact your State and Federal representatives to express your frustration regarding the situation and request a change to requirements for healthcare insurance that would prevent this from happening. This won’t take care of the current claim, but it might lead to change in the future.
Here are two TikToks from my personal experience navigating claims with my private insurer.
Health insurance denials and claim mishandling are something I have experienced for years. These are merely a few. I wanted to get this out for the ABC News report that Dr. Glaucomflecken mentioned but it seems the account is gone.#healthinsurance#healthinsurancedenials#chronicillness#navigatinginsurance @Dr. Erin Nance 🇺🇸 @Dr. Rubin, MD @Dr. Glaucomflecken @ABC World News Tonight @Aaron Parnas @UnderTheDeskNews
Disclaimer. This article is based on research and personal experience. This information is not intended as legal advice or healthcare advice. This is informational and parts not from research or able to be documented in my EOBs/experience with my personal private insurance would be based on my personal opinion.
Disparities across income, education, race, and ethnicity
Hoagland, Yu, and Horny (2024) examined the association between patient demographics and insurance denials for preventive care among a cohort of 1,535,181 privately insured patients seeking preventive care in the US.
What preventive care was considered in this study? Contraceptive administration, breast cancer screening, cholesterol screening, colorectal cancer screening, depression screening, diabetes screening, and wellness visits.
Here is a summary of their findings:
Patients with low incomes (<$30,000 yearly), high school degree or less, and from minoritized racial and ethnic groups experienced higher rates of claim denials. Most frequently these were noncovered service-diagnosis code pairs and billing errors. (What does this mean? People’s access to basic preventive care is different based on their demographic – or income, education, racial, and ethnic background. This is considered inequity)
Income: The lowest income group (<$30,000 yearly) had 43% higher odds of any denial than those in the highest income group (benefit denials and billing errors; statistically significant).
Race and Ethnicity:
Non-Hispanic black patients had 19% higher odds of denials compared with non-Hispanic white patients
Hispanic patients had 16% higher odds of denials compared with non-Hispanic white patients
Asian patients had 54% higher odds of denials compared with non-Hispanic white patients
Education:Differences were not statistically significant
Did practitioners resubmit bills (i.e., file the bill again) after denials?
32.4% of practitioners resubmitted the claims.
What amount was unpaid by health insurance? The mean (average) of the unpaid denied claim was $1395. This was left to patients 92.85% of the time and varied by patient income, race, and ethnicity.
Low-income patients had a higher burden than high-income patients (medians of $412 vs. $365, respectively)
Non-Hispanic black (median $390), Hispanic (median $464), and Asian (median $522) patients each facing higher costs than non-Hispanic White patients (median $357)
Smaller differences between less-educated patients (median $384) compared with those who had more education (median $399)
Financial burden for those with disabilities, chronic illness, and chronic disease
Note. I struggled to find research addressing this topic as a disparity, and I know I am not including everything out there. Please share any additional information in the comments or email me.
Below is a summary of what I found.
Increased chronic health conditions = increased financial burden. The more chronic conditions a person has is associated with an increased financial burden (i.e., increased debt, increased medical debt in collections, and increased out-of-pocket medical costs; Becker, Scott, Moniz, Carlton, & Ayanian, 2022)
Medical debt = worse population health. Medical debt is associated with worse population health (i.e., more days of poor physical and mental health, loss of years of life, higher mortality rates for all; Han, Hu, & Zheng, 2024)
Most (85%) do not file formal appeals (appeal rights vary based on coverage as do the rules; the process can be complicated)
Often those who need to appeal the health insurance decisions use a lot of health services, and may be too sick to advocate for themselves. (There are programs, Consumer Assistance Programs, available to help; however, they don’t exist in all states and Congress hasn’t appropriated funds since 2010.)
Keep in mind that most of this information describes associations between chronic conditions, medical visits, and financial burden. This means that the values of the variables (e.g., chronic health conditions and financial burden) provide information about each other. This doesn’t mean that more chronic health conditions causes more financial burden, BUT it does mean we can predict the financial burden more accurately when we know the number of chronic health conditions a person experiences.
But implementing such policies will take time and working with both State and Federal elected officials.
What can you do in the in the meantime?
Monitor your medical bills
Know your rights
Ask questions
If you don’t understand something your provider puts on a bill OR your insurance company has on the “Explanation of Benefits”, then ask. (You can even ask me)
But please don’t ignore the error. And I understand how exhausting this is. It isn’t easy. It’s frustrating. It is disheartening. It’s overwhelming.
Disclaimer. This post is not medical or legal advice. It is informational in nature with some information regarding the author’s opinion.
In honor of Dyslexia Awareness Month, here is a 1993 article, Dyslexics Overcome Barriers, that I wrote for my high school newspaper.
I interviewed some of the students at school who had dyslexia as well as some of the teachers who were trained in Alphabetic Phonics (an Orton Gillingham based program) and worked with the dyslexic students.
Dyslexics can provide so much insight into their challenges as well as ways to support them, but so often it seems they aren’t asked for their insight. I’ll go over this more in a future blog, but for now, just consider what these students said in 1993.
Disclaimer. This article is from 1993. The knowledge base about dyslexia has expanded much since that time. This post is only to provide historical insight not diagnose or treat.
Rebecca Warner from pqbd.org allowed me to turn the symbol she created for dyslexia into an emoji! I added it to the access and advocacy discord hosted by Nixon Speech and Language, LLC, but we would love to share this with those who have or know someone who has dyslexia!
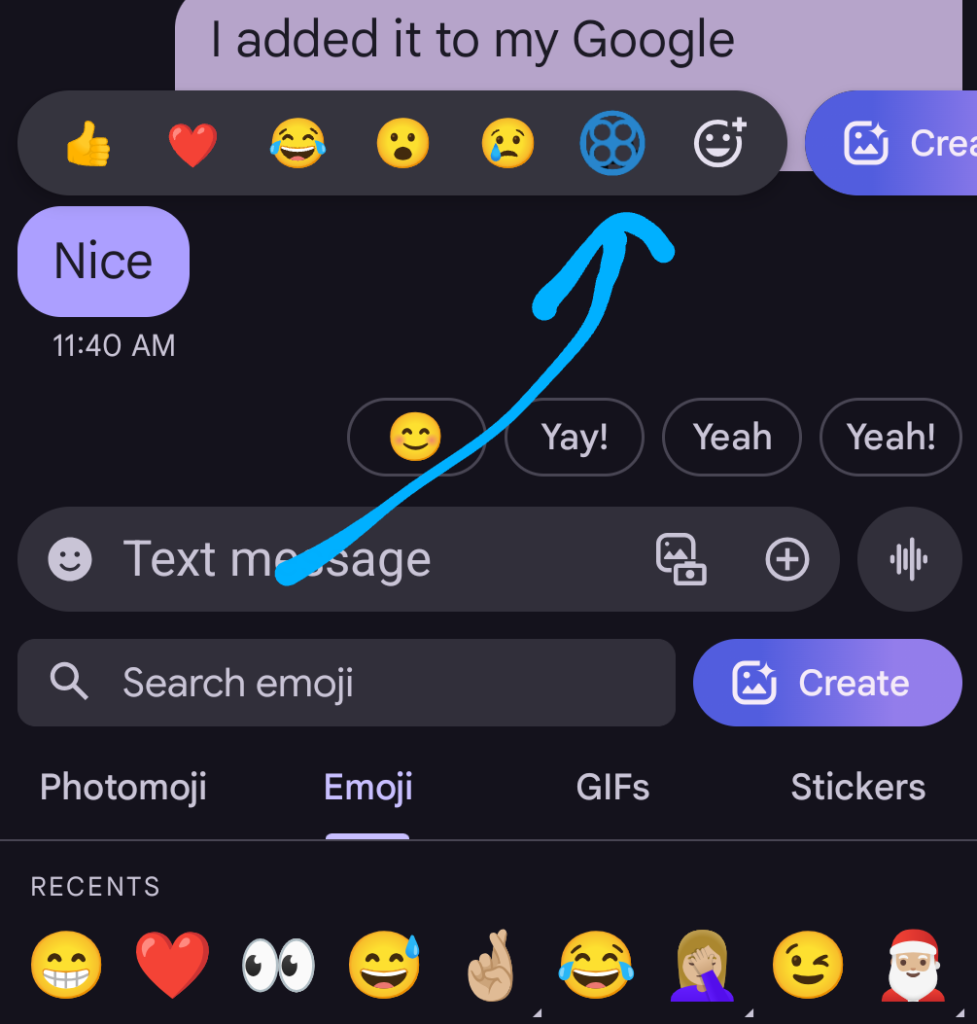
Android Phone Directions
Save the file to your phone and/or a cloud drive you can access with your phone
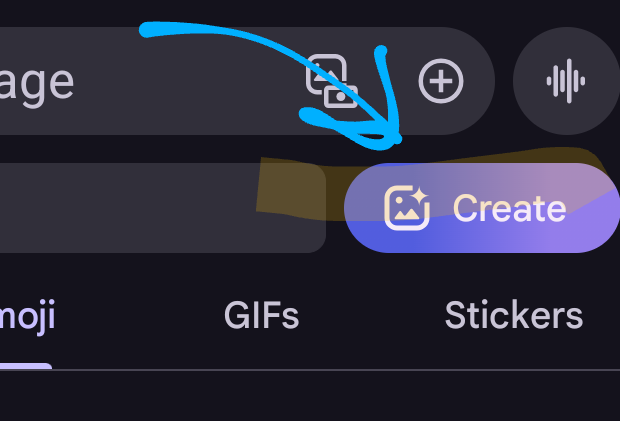
Start a text to someone and select to use an emoji
Select create
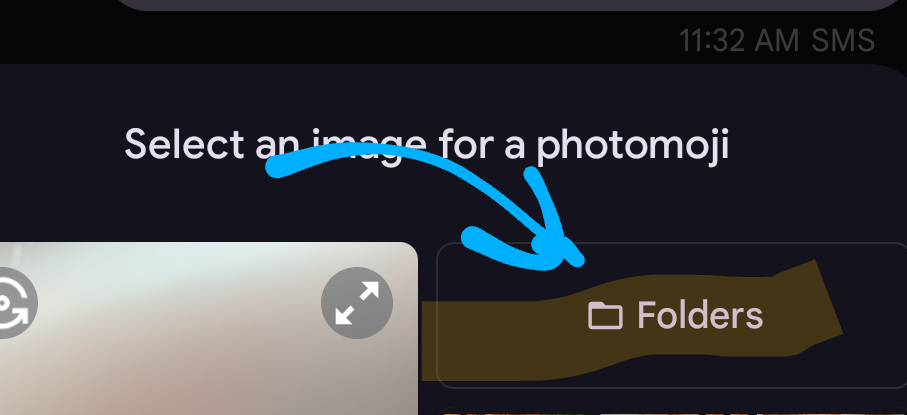
Select folders
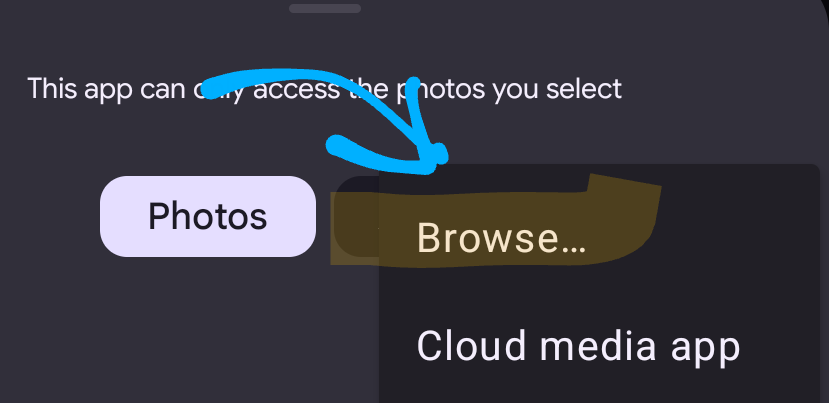
Select browse
Select the file
It will post it to the person you’re texting, but as you can see in the image, it is useable as a react to a text!
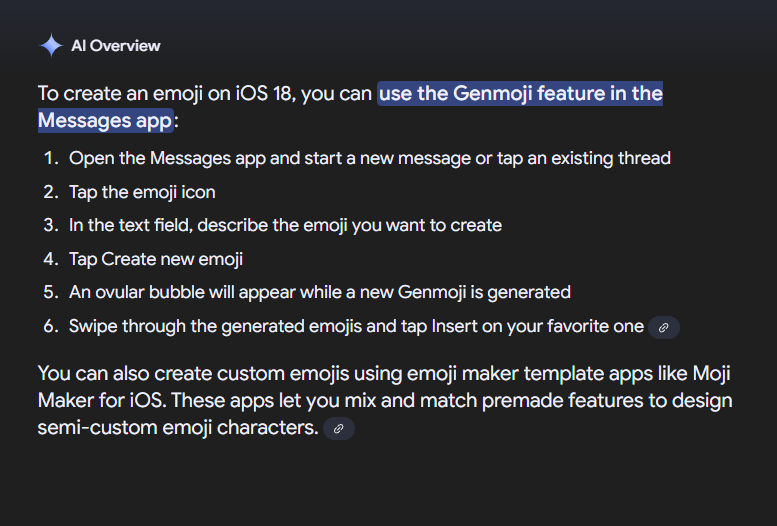
iOS 18 Directions
This description is taken from Google AI Overview. If someone could send me screengrabs as they create the file, then I would be grateful!
My understanding is this is only available for iOS18, but if you learn otherwise, please comment below!
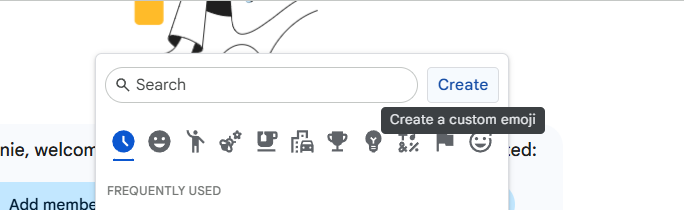
Gmail and Google Workspace Directions
Within gmail, open google chat
Select emoji
On the right, select create
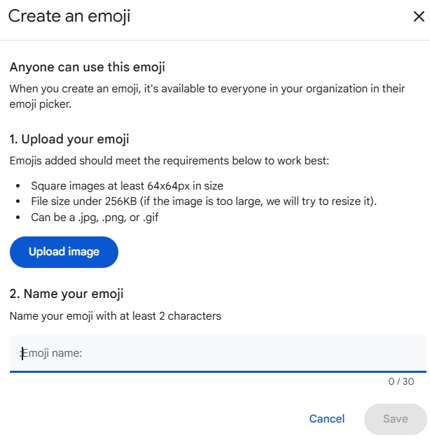
Upload the image file
Name it pqbd dyslexia
Now you can use the file in your emails and chats!
Note. For Google Workspace, staff need permissions to “create” new emojis. So, if you are unable to create one following these instructions, then ask a network administrator.
Thank you to Rebecca Warner and pqbd.org for making this symbol available to everyone!
Rebecca Warner is a 2012 founding member of the Virginia chapter of Decoding Dyslexia, DDVA. Active in legislative efforts in the VA General Assembly as well as a co-host for DDVA meetings, her experience includes speaking engagements, fundraising, and events. Owner and designer of the dyslexia symbol pqbd ®, she advocates for awareness and training in dyslexia both on a national and international level with projects that include the Dyslexia Friendly Library, Police National Dyslexia Association in the UK, Learning Disabilities Conference Japan, Dyslexia Organization Kenya, and the marketing committee for Riverside School. Most importantly, she is the mother of two neurodiverse sons, a dyslexic junior at Rose-Hulman Institute of Technology and an ADHD sophomore at the University of Virginia. She and her husband live in Richmond, VA.
You know those moments you wonder whether others have dealt with the challenge you (or anyone you care about) are facing? Maybe they have an idea you haven’t thought of? Or maybe you just don’t know what to do next?
We can learn from each other by sharing information, particularly when it comes to disability access and advocacy. To improve outcomes for individuals facing those barriers, we need to bring the stakeholders to the conversation.
To get these conversations started, I have started a discord. I know some people may be less familiar with discord, so don’t worry, I’ll do my best to guide those who don’t have discord yet.
Some quick notes that will help you get started:
Joining as an individual/caregiver? I’d recommend NOT using your real name or picture just to protect your privacy. I have information about this in the channel called “Setting up a Discord Profile”
Joining as a professional? (Educator, provider, advocate/attorney) If you are representing your profession, then use your name. (If you have a gaming discord though, you may want to create a discord account specifically for professional purposes.)



{kind=link}
Leave a Reply