Many people talk about university researchers as living in the “ivory tower” unaware of the needs of people in society.
I challenge you to pause for about 10 minutes and watch this video courtesy of PBS News to better understand potential long-term impacts of Trump’s cuts to research funding.
(And yes, I know the video is about medical research funding, but the same applies to education. Also, NIH funds more than medication research. They fund research into child development, reading, language, speech production, and so much more.)
PBS News Hour clip about Trump’s cuts to medical research funding (2025). This is a wonderful summary.
Beyond that video, did you know that research grant funds also help pay tuition for students working in those labs? Yes. They can make higher education more affordable.
It’s part of the reason most grad and doctoral students look for labs with funding.
If research funding is decreased, then we may end up with less socioeconomic diversity in higher education due to the cost.
If research funding is decreased, then students who choose to pursue higher education degrees are likely to have higher student debt.
What can you do?
Contact your representative and senator
Speak UP! Post on social media!
Disclaimer. Information provided in this post by, Stephanie M. Nixon, Ph.D., CCC-SLP, is provided in good faith. Nixon Speech and Language, LLC makes no representation or warranty of any kind, express or implied regarding the accuracy, adequacy, validity, reliability, availability, or completeness of any information supplied by other sources.
Information provided here is for informational purposes only.
If you don’t need this article to realize the necessity of the Institute of Education Sciences (IES) and their role in funding high quality independent educational grant research, then please sign this petition in an effort to halt actions by DOGE and the current Presidential administration: https://chng.it/vjdYGZw9wz
If you just need the numbers to sign the petition:
2024 entire Federal Budget was $6.75 trillion.
IES had an $807 million budget in 2024
Between $800 million and $1 billion in IES research grants were cut by DOGE (Grants are paid over multiple years. See the note below.)
Note. In this Washington Post Article posted 2/13/2025 by Meckler and Natanson, Nat Malkus, a senior fellow at American Enterprise Institute DOGE may have overstated the cost of the canceled contracts because many of the contractors were several years into the agreements, meaning the money has already been spent.
In other words, canceling the grants right now likely caused more waste, especially if the studies cannot be completed due to lack of funding.
Other reasons to sign:
IES is part of the accountability arm of the education system
Studies are being cut short including one called, ReSolve designed to help students learn math faster.
Federal funding cuts including grant funding to researchers at the institutions is devastating. This article in the GW Hatchet by Jenna Lee (2/11/2025) addresses lawsuits related to the NIH Federal funding cuts
DOGE cut additional resources within that funding including:
Common Core of Data, primary database of all K-12 schools with enrollment, demographics, and other information is collected
What Works Clearinghouse: a project that has been essential to facilitating decisions for administrators and educators (see below for more)
School Pulse Panel: began surveying K-12 public schools about education related topics
Studies about international education
Career and technical education
Early childhood education
Contact your congressmembers. Protect this funding so our country can move forward with improving our education system on the whole vs. backwards. We need independently funded research. It is paramount.
I posted this in a previous post, and I’m posting it again.
If you need more convincing or just want some background, then read on.
Briefly…why do we have a Federal Department of Education?
Before we can discuss the Institute of Education Sciences (IES), we need to consider, why do we have a Federal Department of Education (DoEd)? Can’t the states do everything?
Time machine:
Let’s hop in our “time machines” and review history:
Non-cabinet level agency with Henry Barnard as the first commissioner (and a staff of 3 and only 2 rooms)
Objectives:
improve American education by providing strong education information to local- and state-level authorities without having official control of the authorities in the states
collect statistics and facts to show educational progress across states and territories
Henry Barnard
He deserves his own post (if I have time). For now, review the Barnard Papers and the information from Cross and Islas. Barnard had to collect data from the schools and send it to practitioners. He and his small staff produced reports and research to help give a context for education.
July 20, 1868: Congress decided the the efforts by Barnard was a waste of national resources, reduced the funding, and then on June 30, 1869 removed the DoEd’s independent status and relabeled it the Office of Education with the Department of Interior.
1870:John Eaton served as the US Commissioner of Education until 1886 with only a $6000 yearly budget.
1889 to 1906: Commissioner William Torrey Harris continued the data collection and expanded it to include public and private elementary school enrollment.
This path continued, the name changed and shifted. In 1953, the Department of Health, Education, and Welfare. More funds were available due to political and social circumstances.
In 1963, President Lyndon B. Johnson emphasized the need for education to fight poverty leading to the Higher Education Act (1965) and Elementary and Secondary Education Act (1965).
Now, it’s 1979, President Jimmy Carter signed into law the Department of Education Act
This established the Federal Department of Education as a cabinet-level department.
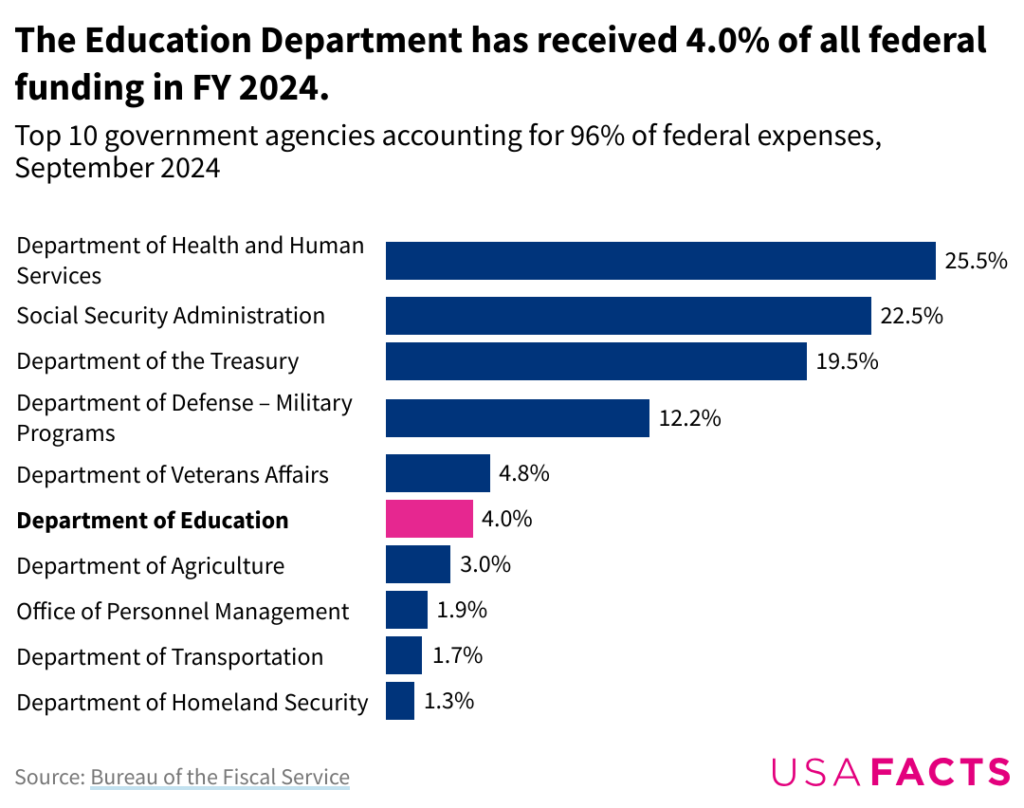
What kind of funding did DoED receive in 2024?
Per USAfacts.org, DoED received 4% of all federal funding in 2024, totaling $268.35 billion.
Originally posted by USA FACTS.
DoEd is the smallest of any cabinet-level department with about 4,100 full-time employees (as of 2023).
What is/was the function of DoEd as of 2024?
Note. Given the unknowns related to what data/websites will remain available under the current administration, I cannot guarantee the existence of any links to federal websites. If you click a link and it is gone, then please contact me and I will do what I can to find the information and make it accessible (when possible).
“Strengthen the Federal commitment to assuring access to equal educational opportunity for every individual;
Supplement and complement the efforts of states, the local school systems and other instrumentalities of the states, the private sector, public and private nonprofit educational research institutions, community-based organizations, parents, and students to improve the quality of education;
Encourage the increased involvement of the public, parents, and students in Federal education programs;
Promote improvements in the quality and usefulness of education through Federally supported research, evaluation, and sharing of information;
Improve the coordination of Federal education programs;
Improve the management of Federal education activities; and
Increase the accountability of Federal education programs to the President, the Congress, and the public.”
As noted on the about page for DoEd, the mission “is to promote student achievement and preparation for global competitiveness by fostering educational excellence and ensuring equal access for students of all ages. Learn more about our mission, offices within ED, key initiatives, and more.”
What is the Institute of Education Sciences (IES)?
promotes high quality comprehensive research to expand knowledge of children and youth with or at risk for disabilities
age range is infancy through post-secondary education
ERIC: Repository of education related information including journal articles, dissertations, and other such resources
Importance of IES
IES is how we improve education. Under this institute, there have been education advances. Chester Finn wrote commentary on February 12, 2025 about this current situation with funding cuts to IES by DOGE. IES in its current form “corrected much of what was weak and wasteful in the previous arrangement —and the new agency got off to a strong start under the leadership of Grover (Russ) Whitehurst, who strove with considerable success to see that its work would be conducted as proper scientific research—controlled experiments, etc.—and data gathered and reported with objectivity and integrity”.
Information for this post was pulled from these webpages (citations also linked within the post itself as appropriate):
Disclaimer: Including these links is not intended as Nixon Speech and Language, LLC’s or my an endorsement OR agreement with information created by the authors, companies, institutes, or websites. If you find factually inaccurate information in my post or a link, then please let me know and I will adjust.
Disclosure. I am writing this as a supporter of strong education science and research. I am writing this as educators need rigorous peer-reviewed randomized studies to facilitate decisions. In my opinion, they also need access to quickly disseminated information as is available in What Works Clearinghouse. I am concerned at the likely negative outcomes for all children, but particularly those with learning disabilities or at risk for learning disabilities.
I worked at the Institute of Education Sciences from January 2004 through about March 2005 in the National Center for Education Research. I saw the amazing research. I watched the peer reviews.
Disclaimer. Information provided in this post by, Stephanie M. Nixon, Ph.D., CCC-SLP, is provided in good faith. Nixon Speech and Language, LLC makes no representation or warranty of any kind, express or implied regarding the accuracy, adequacy, validity, reliability, availability, or completeness of any information.
The opinions expressed in this post, are exactly that, opinions of Stephanie M. Nixon, Ph.D., CCC-SLP.
Note. This is an updated version of an article I wrote in 2021 for Apraxia Kids. The main reference was to childhood apraxia of speech research, but this applies to research across the sciences.
Some current (2025) actions by the executive branch make information of utmost importance. Some changes threaten sources of independent research funding.
What is evidence-based practice?
You may have heard speech-language pathologists (SLPs) saying “evidence-based practices” when describing a specific treatment approach. Such practices are based on scientific evidence and professional experience while considering your child’s specific needs.
Scientific evidence is used by SLPs, educators, and medical professionals (among others) to guide interventions and strategies could help a person based on their specific needs.
There is not one approach that works for all people, especially not for all children with childhood apraxia of speech (CAS). There are some approaches that have not been studied at all or have been studied with research methods that don’t allow for very strong conclusions.
What is scientific evidence?
Scientific evidence is empirical data that is collected and interpreted using the scientific method. This is evidence that serves to support or counter a scientific theory or hypothesis and is derived from controlled studies.
Is all scientific evidence high quality?
Simply put, no.
Well-designed research studies are more valuable tools than an anecdotal opinion.
What are the levels of evidence?
Additional information about evidence-based interventions as defined in the Every Student Succeeds Act (ESSA) from the California Department of Education.
Let’s summarize…
The lowest form of evidence = opinions based on “experience”
Best form of evidence = pulling multiple randomized controlled trials into guidelines or a meta-analysis
Anecdotes are not evidence especially when these anecdotes are offered by (or on websites of) people/companies with a commercial interest.
Note. Researchers/organizations obtain grant funding by applying. Even then, there is a review process to determine whether they receive the funding.
Applications are peer reviewed by field experts who determine whether the application meets the criteria among other standards.Why does commercial interest matter in speech-language pathology or education?
What is a commercial interest? Earning money by selling a product OR saving money by not providing a service. (The latter is more relevant to health insurance – at least for now.)
Example: Dr. Blah at company XYZ creates and markets a program to teach math. If it is sold to school districts, then they will make money. Now if XYZ and Dr. Blah are the only ones who research the program they are more likely to determine this “works”.
What can decrease the quality of evidence?
Specific to CAS treatment research studies, look for study limitations (e.g., small sample size, inconsistent implementation of treatment approach, lack of a control group or condition, pre-treatment differences between groups, analysis performed by non-blinded outcome assessors, etc.).
Do we have much of the Level 1 standard research for Childhood Apraxia of Speech treatment?
No. We have a few meta-analysis studies and systematic reviews available.
Here are some systematic research reviews (most summaries by the American Speech Language Hearing Association in their Evidence Maps):
Murray, McCabe, and Ballard (2014) concluded that of the research articles they analyzed, at least 3 treatments had sufficient evidence for Phase III clinical trials. Those treatments were Dynamic Temporal and Tactile Cueing (DTTC), Integrated Phonological Awareness, and Rapid Syllable Transition Treatment.
Ng, McCabe, et al. (2022) found an evidence base for the use of Rapid Syllable Transition Treatment (ReST).
Springle, Breeden, et al. (2020) found limited higher dose and frequency of motor programming treatments appeared most effective for children with CAS.
SLPs can look at the “evidence” to determine which approaches are most likely to work. The evidence includes the research available and the patient’s unique needs.
What characterizes a strong treatment research study?
Diversity in the population? (i.e., Gender? Race? Ethnicity? Primary language? Age – depending? Diagnoses? Socioeconomic status (SES)? Geographic location? Gender identify and expression? Disability status?)
Why do we care about diversity in the sample ?
Simply put: Inclusivity matters. The linked 2023 article by Alice McCarthy details the need for inclusive clinical trials.
Yes, we’re dealing with speech-language therapy trials vs. drug trials; but, that doesn’t change the need to ensure a representative population. This might advise a research of possible barriers to care as well as how to address the barriers.
Randomization: There are many types of randomization as described in the article linked (Lim & In, 2019). Randomization helps researchers eliminate/minimize accidental bias (including selection bias).
e.g., We want to ensure that patients weren’t chosen to receive the “treatment” group merely because they seemed to have more or less speech sound errors.
Bias in research
Bias in research is beyond the scope of this article. If you’d like to learn more, here is one journal article by Pannucci and Wilkins (2010).
Internal consistency indicates that several items measuring the same idea generate similar responses.
External consistency is the degree to which results are consistent with prior research.
Specific to consistency of analysis, we want to know how reliable were measures of patient performance. What was the level of agreement between/among therapists? How about a novel therapist?
Were the control and treatment interventions provided as intended? For example, did the SLPs administering the interventions stay within the guidelines provided by the research study? Did they introduce any concepts not included in the study?
Was the same modality of treatment used across patients in each condition? (in-person, telehealth, etc.)
Example.
(1) SLP working with a child in the “control” group includes some of the techniques from the “treatment” being tested and child shows progress in the “control” intervention.
Does this mean the “control” intervention works? No. It means the SLP did not follow the research protocol in the “control” intervention.
(2) SLP working with a child in the “treatment” group includes techniques beyond those described by the researchers as part of the treatment program (e.g., visual aids, cues, etc.) and the child shows progress with the “treatment” intervention.
Does this mean the “treatment” intervention works? No. It means the SLP did not follow the research protocol in the “treatment” intervention.
Other important factors
We also need to consider the presence of other factors that could explain improvement or regression (including whether these were controlled in the study). and whether these are controlled (e.g., if a child also received treatment elsewhere, or if a child started school, or had a medical procedure).
Was the child receiving treatment beyond that supplied in the study?
Did the child start school while in the study?
Did the child experience any medical changes during the study? (e.g., new medication, surgical procedure, new diagnoses, accident, etc.)
Maturation(i.e., getting older) is another factor to consider when reviewing treatment studies. That is, did the treatment group improve beyond what would be expected based with aging.
What if one approach with research support isn’t working for my child?
Well, if you have that concern, ask the practitioner. Practitioners usually track progress so they know when they need to adjust intervention (i.e., when the approach is not effective for the patient or when the patient masters an objective, etc.).
As a clinician, I ask myself these questions when an approach doesn’t seem to be “working”?
How long have we tried the approach?
Am I implementing the approach correctly? (It helps to review the approach.)
Is the child engaged (i.e., attending) with us during our sessions?
How consistent is the child’s attendance?
Have we provided appropriate family education (if included) with the approach? (This includes home practice)
Sometimes an approach just isn’t the best option for a child (and their family) and we need to adapt. This could include modifying the approach slightly to adapt or even changing approaches to one more suited for the child.
Regardless, an approach should have an evidence base, even if it was only demonstrated in a “single-subject design case study”. This allows SLPs to generate ideas/hypotheses (sophisticated educated guesses) about what might work for a given child.
Disclaimer. Information provided in this post by, Stephanie M. Nixon, Ph.D., CCC-SLP, is provided in good faith. Nixon Speech and Language, LLC makes no representation or warranty of any kind, express or implied regarding the accuracy, adequacy, validity, reliability, availability, or completeness of any information.
Information provided here is for informational purposes only.
This material is not substitute for professional medical advice or treatment. Always seek the advice of a qualified professional with any questions you may have regarding conditions and treatments/therapies. Do not delay seeking professional medical or educational advice/evaluation or delay seeking it because of something you read on this website.
See these websites for more information about evidence-based practices and research:
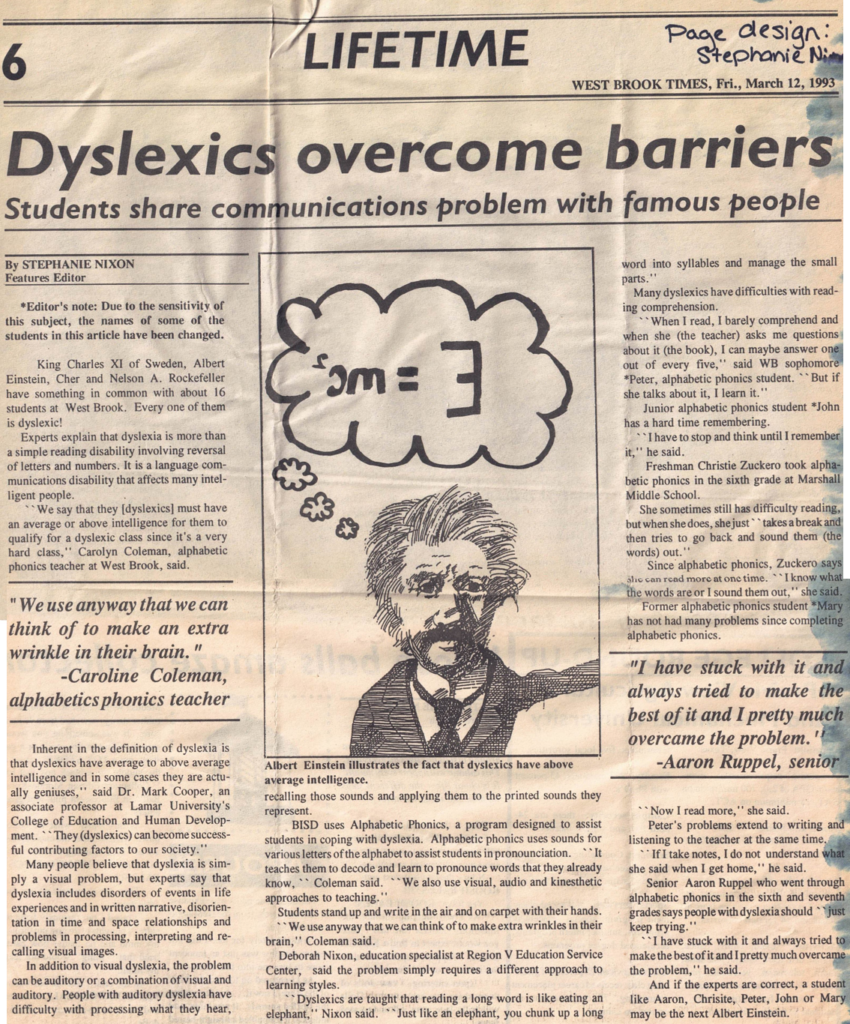
In honor of Dyslexia Awareness Month, here is a 1993 article, Dyslexics Overcome Barriers, that I wrote for my high school newspaper.
I interviewed some of the students at school who had dyslexia as well as some of the teachers who were trained in Alphabetic Phonics (an Orton Gillingham based program) and worked with the dyslexic students.
Dyslexics can provide so much insight into their challenges as well as ways to support them, but so often it seems they aren’t asked for their insight. I’ll go over this more in a future blog, but for now, just consider what these students said in 1993.
Disclaimer. This article is from 1993. The knowledge base about dyslexia has expanded much since that time. This post is only to provide historical insight not diagnose or treat.
Rebecca Warner from pqbd.org allowed me to turn the symbol she created for dyslexia into an emoji! I added it to the access and advocacy discord hosted by Nixon Speech and Language, LLC, but we would love to share this with those who have or know someone who has dyslexia!
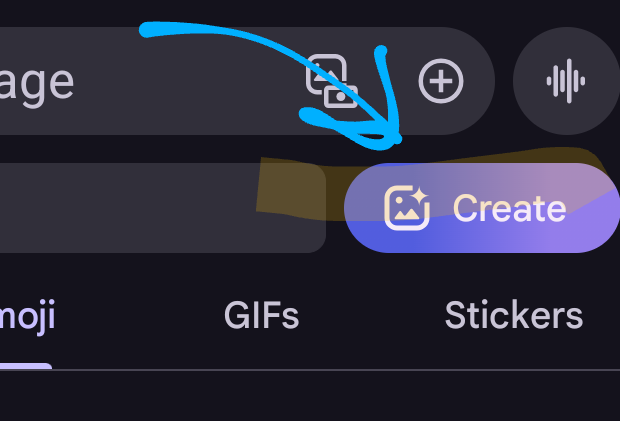
Android Phone Directions
Save the file to your phone and/or a cloud drive you can access with your phone
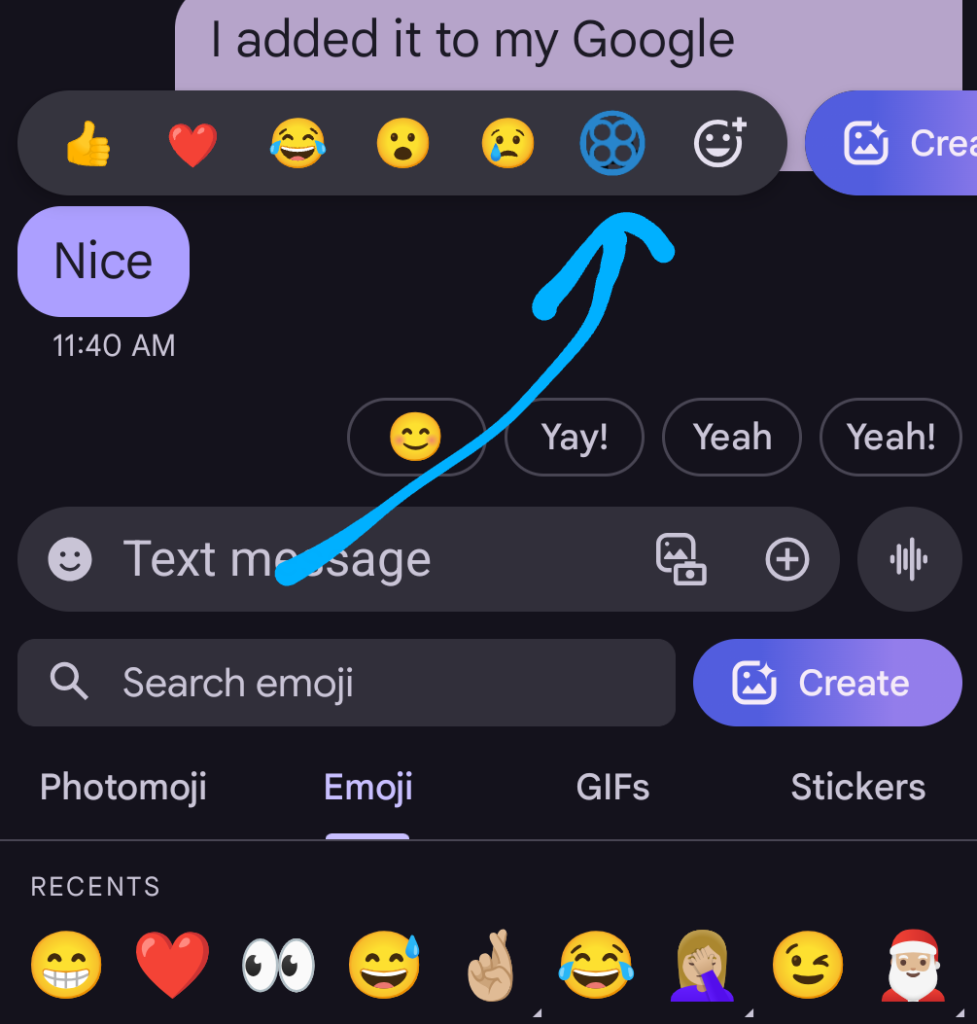
Start a text to someone and select to use an emoji
Select create
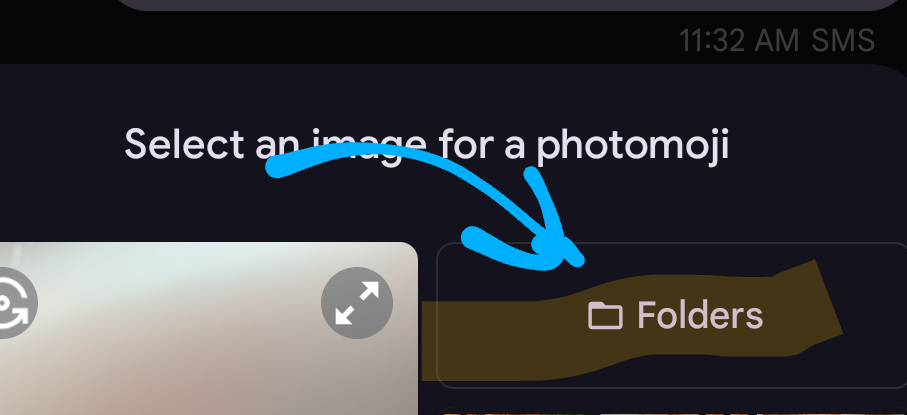
Select folders
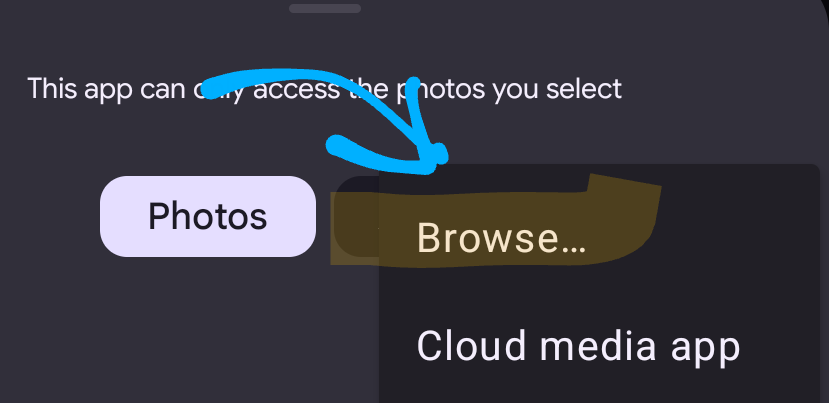
Select browse
Select the file
It will post it to the person you’re texting, but as you can see in the image, it is useable as a react to a text!
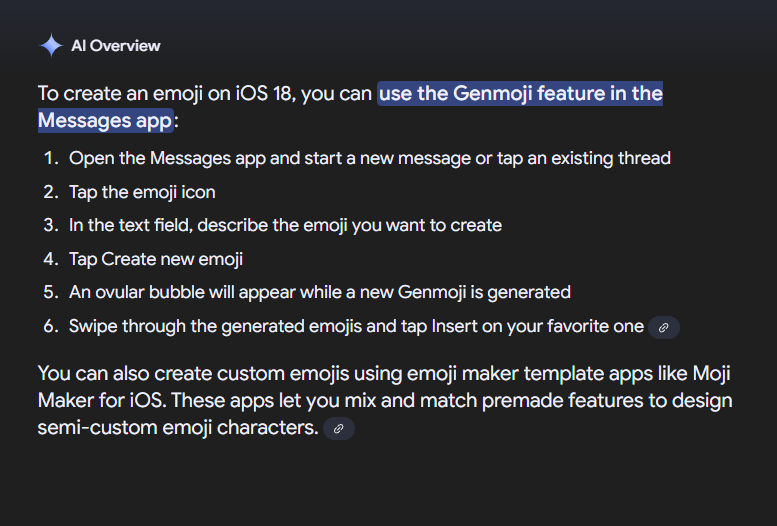
iOS 18 Directions
This description is taken from Google AI Overview. If someone could send me screengrabs as they create the file, then I would be grateful!
My understanding is this is only available for iOS18, but if you learn otherwise, please comment below!
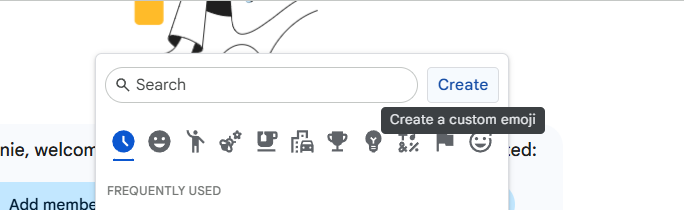
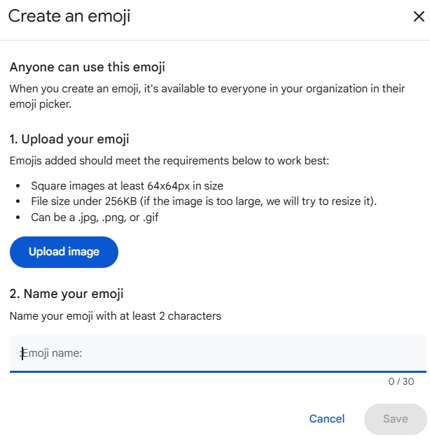
Gmail and Google Workspace Directions
Within gmail, open google chat
Select emoji
On the right, select create
Upload the image file
Name it pqbd dyslexia
Now you can use the file in your emails and chats!
Note. For Google Workspace, staff need permissions to “create” new emojis. So, if you are unable to create one following these instructions, then ask a network administrator.
Thank you to Rebecca Warner and pqbd.org for making this symbol available to everyone!
Rebecca Warner is a 2012 founding member of the Virginia chapter of Decoding Dyslexia, DDVA. Active in legislative efforts in the VA General Assembly as well as a co-host for DDVA meetings, her experience includes speaking engagements, fundraising, and events. Owner and designer of the dyslexia symbol pqbd ®, she advocates for awareness and training in dyslexia both on a national and international level with projects that include the Dyslexia Friendly Library, Police National Dyslexia Association in the UK, Learning Disabilities Conference Japan, Dyslexia Organization Kenya, and the marketing committee for Riverside School. Most importantly, she is the mother of two neurodiverse sons, a dyslexic junior at Rose-Hulman Institute of Technology and an ADHD sophomore at the University of Virginia. She and her husband live in Richmond, VA.
You know those moments you wonder whether others have dealt with the challenge you (or anyone you care about) are facing? Maybe they have an idea you haven’t thought of? Or maybe you just don’t know what to do next?
We can learn from each other by sharing information, particularly when it comes to disability access and advocacy. To improve outcomes for individuals facing those barriers, we need to bring the stakeholders to the conversation.
To get these conversations started, I have started a discord. I know some people may be less familiar with discord, so don’t worry, I’ll do my best to guide those who don’t have discord yet.
Some quick notes that will help you get started:
Joining as an individual/caregiver? I’d recommend NOT using your real name or picture just to protect your privacy. I have information about this in the channel called “Setting up a Discord Profile”
Joining as a professional? (Educator, provider, advocate/attorney) If you are representing your profession, then use your name. (If you have a gaming discord though, you may want to create a discord account specifically for professional purposes.)







{kind=link}
Leave a Reply