Patient Track: Being good at makeup, didn’t mean I was well.
Disclaimers.
Professional Standards and Scope:
Credentials and expertise: Dr. Stephanie Michelle Nixon is a PhD-level Speech-Language Pathologist and consultant.
Educational purpose: The content in this series is shared for informational, educational, and advocacy purposes only.
No clinical relationship: Engagement with this content does not constitute medical advice, a clinical diagnosis, or the establishment of a patient-provider relationship.
Medical consultation: Always seek the advice of your physician or other qualified health providers with questions regarding a medical condition.
Personal Narrative & Data Integrity:
Designated Record Set: This series represents a personal, professional audit of my own legally obtained medical history and “Designated Record Set”.
Factual Basis: All clinical data points—including the 169.4-minute gastric emptying result —are pulled directly from my documented clinical records.
Advocacy Intent: My goal is to highlight systemic disparities in medical documentation and foster better clinical communication.
Non-Defamation: This audit is a critique of the content and quality of documentation and the patterns of clinical bias, rather than an attack on specific individuals or institutions.
A Note on Neurodivergent Baseline:
Contextual Accuracy: Observations regarding communication style, energy, or behavior (often labeled “manic” or “pressured” in my records) must be viewed through the lens of my documented, lifelong ADHD diagnosis.
A ‘u’ was added (AuDHD) as a late diagnosis a few years ago providing a key to understanding why so many providers saw ‘manic’ behavior where there was actually just a neurodivergent person managing a health emergency. We have to stop labeling what we don’t understand.
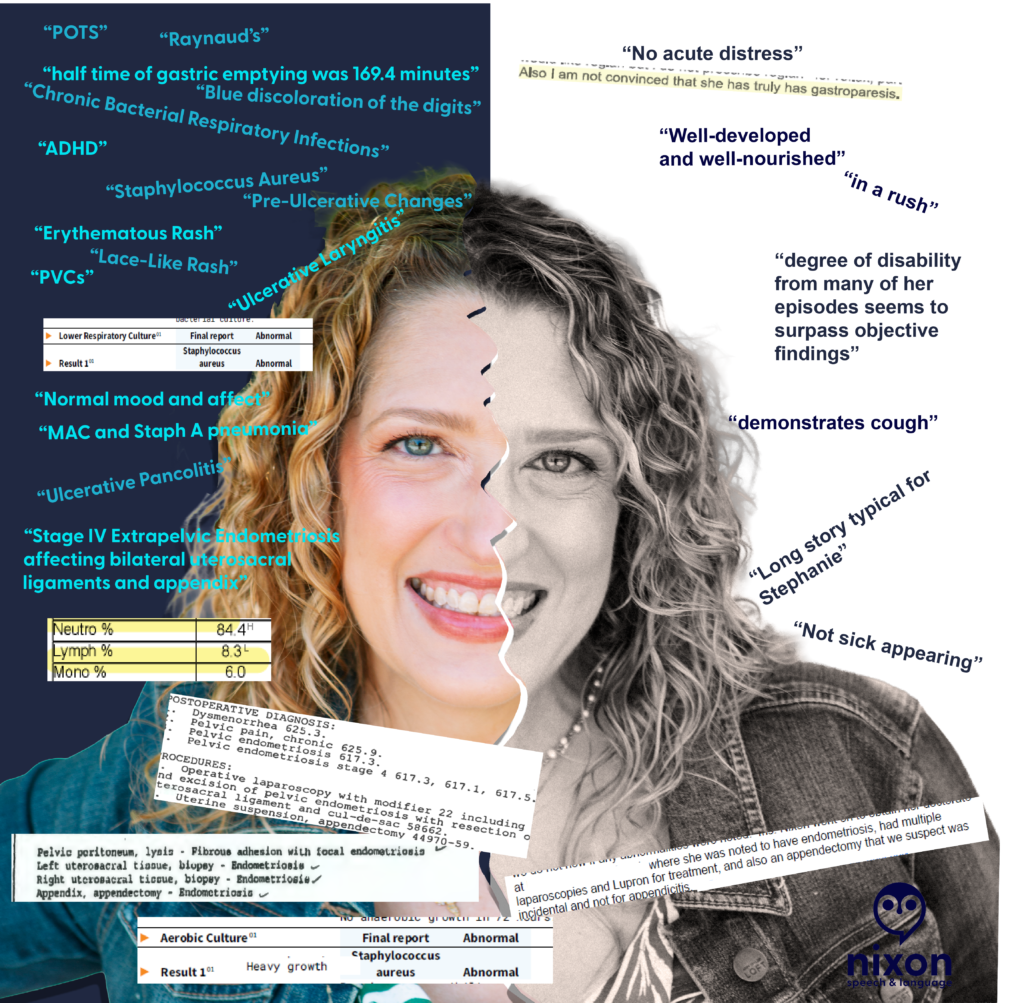
Which version of you is in your medical record? On the right are the labels found in my permanent charts—words like “typical,” “rushed,” “not sick appearing”, “well groomed”. On the left is the objective data my body was reporting at that exact same time.
Words have weight. After auditing my own medical charts across different institutions, it became obvious just how much weight those words carry—and how they can shadow a patient for decades. And let me say, words can hurt.
During an initial appointment years ago, a provider looked at me and said, “You look well.” My response came quickly: “I’m good at makeup.”
How many of us get up, put on our “mask” (a smile, our makeup, shallow breaths to avoid a cough), and go about our day? I know I did. I watched TikToks to improve my makeup skills while I was getting sicker. I didn’t want the world to see me looking as bad as I felt.
But do we really need to look as bad as we feel for a provider to believe the data? I once showed a provider a photo of myself before I put on my makeup that morning, just so she could see the reality of my physical state. Her response? “Why are you showing me this?”
Looking back, I realize that if a provider needs you to look “sick enough” to believe your symptoms, they aren’t the right provider for you.
Receipts
The Science: A specialist was “not convinced” I had a condition, despite a nuclear study providing a 169.4 minute gastric half-time – nearly double the normal limit.
The “Well-Appearing” Paradox: My chart once documented me as “well-appearing” and in “no acute distress” while my oxygen saturation was recorded at 65% at room air. (Note. The 65% was likely associated with PVCs.)
The “Performance” Label: My cough was described as something I “demonstrated” when I was actually navigating multiple bacterial respiratory infections (including … MAC and Staph).
The Missing “u”: My speech was labeled as “pressured,” a psychiatric term that completely ignored my AuDHD baseline (ADHD 1979 / Autism 2024; iykyk).
Audit Your Medical History
Have you ever found a statement in your records that felt more like a character critique than a clinical note?
What is one “label” a provider gave you that was the complete opposite of your reality?
How did it change the way you presented yourself at your next visit?
Provider Track: Would you want these words in your permanent record?
Disclaimers.
Professional Standards and Scope:
Credentials and expertise: Dr. Stephanie Michelle Nixon is a PhD-level Speech-Language Pathologist and consultant.
Educational purpose: The content in this series is shared for informational, educational, and advocacy purposes only.
No clinical relationship: Engagement with this content does not constitute medical advice, a clinical diagnosis, or the establishment of a patient-provider relationship.
Medical consultation: Always seek the advice of your physician or other qualified health providers with questions regarding a medical condition.
Personal Narrative & Data Integrity:
Designated Record Set: This series represents a personal, professional audit of my own legally obtained medical history and “Designated Record Set”.
Factual Basis: All clinical data points—including the 169.4-minute gastric emptying result —are pulled directly from my documented clinical records.
Advocacy Intent: My goal is to highlight systemic disparities in medical documentation and foster better clinical communication.
Non-Defamation: This audit is a critique of the content and quality of documentation and the patterns of clinical bias, rather than an attack on specific individuals or institutions.
A Note on Neurodivergent Baseline:
Contextual Accuracy: Observations regarding communication style, energy, or behavior (often labeled “manic” or “pressured” in my records) must be viewed through the lens of my documented, lifelong ADHD diagnosis.
A ‘u’ was added (AuDHD) as a late diagnosis a few years ago providing a key to understanding why so many providers saw ‘manic’ behavior where there was actually just a neurodivergent person managing a health emergency. We have to stop labeling what we don’t understand.
medical gaslighting and the importance of accurate, data-driven medical records for neurodivergent (AuDHD) patients." class="wp-image-967" srcset="https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-1024x1003.png 1024w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-300x294.png 300w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-768x752.png 768w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-1536x1505.png 1536w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-2048x2006.png 2048w" sizes="(max-width: 1024px) 100vw, 1024px" />
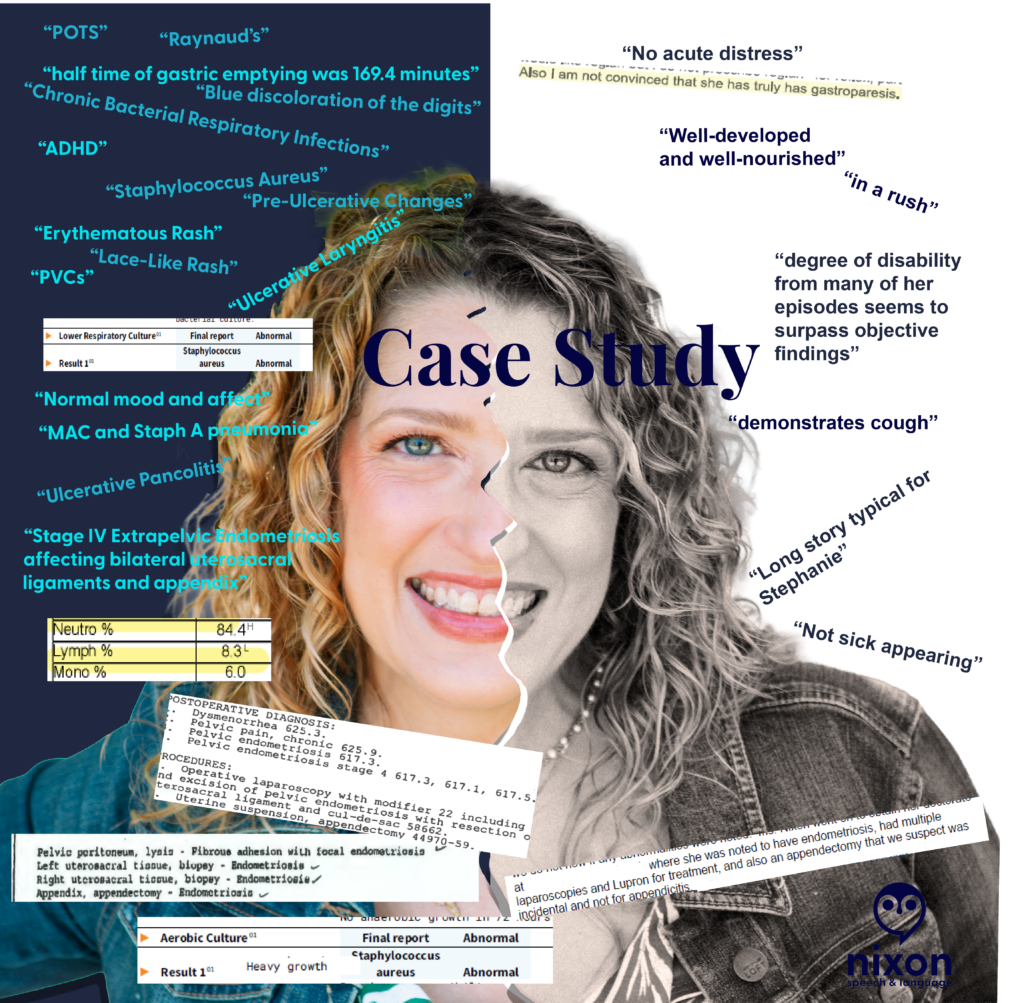
Clinical documentation is a record of pathology, not a character assessment. Yet, after auditing my own medical records, I found decades of “subjective” notes that had nothing to do with my physiological state and everything to do with a provider’s snap judgement and dismissal of my lived reality.
It doesn’t matter if a provider feels these words “justified” in the moment. Once they are in the patient’s chart, they become a permanent filter for every provider who follows.
The words on the black and white side minimize and dismiss both objective findings and my symptoms.
In the image above, a provider documented that my degree of disability ‘surpassed objective findings.’ In doing so, they failed to recognize my functional reality: I was a Speech-Language Pathologist unable to see my patients for 3 weeks after losing my voice to an ulceration on my vocal fold. When documentation focuses on ‘surpassing findings’ but ignores a total loss of vocational function, the clinical record is incomplete. We must document the patient’s life, not just the provider’s impression.
The Scope-of-Practice Gap:
I found repeated psychiatric judgments—labels like ‘pressured speech’ and ‘somatization’—written by specialists who were not psychiatrists or behavioral neurologists. Labeling a communication style as ‘pressured speech’ without establishing a neuro-informed baseline (AuDHD) isn’t just a misinterpretation—it is a specialist overstepping their scope to pathologize a natural speech rate instead of investigating physical health.
What they called “pressured”:
A Neurodivergent Baseline: If anyone had paused to ask, I would have laughed and told them that I had the words “SLOW DOWN!” in bold on every note for every presentation during my post-graduate education.
Physiological Distress: Rapid speech and “short rushes” are frequently associated with shortness of breath. Documentation that reaches for a psychiatric label while a patient is in respiratory distress is a failure of clinical reasoning.
Fluency Dynamics: As an SLP, I recognize these patterns as potential symptoms of cluttering among other speech and language disorders.
None of these clinical presentations require a mental health diagnosis. When we reach for mental health labels to describe a fast speech rate, we ignore the very real physical or fluency-based realities of the patient standing in front of us.
The “Incidental” Dismissal
I once had a specialist (not a gynecologist or GI) dismiss my appendectomy as “incidental” to my laparoscopy for Stage IV extra-pelvic endometriosis. When a pathology report confirms ‘Appendix – Endometriosis,’ that appendectomy is a diagnostic data point, not an ‘incidental’ event. Labeling it as such signals to every future provider that the patient’s surgical history—and their reported pain—is irrelevant.
The Receipts:
The Science: A 169.4-minute gastric half-time (normal is <90) was dismissed by a specialist who was “not convinced.”
The Paradox: A 65% O2 saturation reading was recorded alongside a note that I was “well-appearing”. (Note. The 65% O2 reading was likely associated with PVCs based on the other data in the visit.)
The Shorthand: A systemic crisis involving a 20-lb weight gain and pitting edema was labeled “long story typical for Stephanie”.
The Challenge:
The Mirror Test: If you were the patient, would you want a crisis described as “typical” for you?
Stay in Scope: If you aren’t a psychiatrist, why are you reaching for psychiatric labels to describe a patient’s communication? (Also, check with the patient. Had that provider asked me, I would’ve laughed and told her that my rate of speech has always been fast…in fact, I must actively think about it to speak more slowly.)
Watch for Bias: Literally watch for it. If you see a dismissive note from a colleague, don’t carry it forward. Check the data, ask the patient, and document the objective truth.
Let’s hold the record to a higher standard. How can we ensure our “Subjective” notes don’t do lasting harm?
🚨 TL;DR: The “Paddle Boarder’s Guide to Surviving the Medical System”
The Problem: For neurodivergent and chronically ill people, a change in medical plans (like a surgery delay) isn’t just an “inconvenience.” It is an enormous, destabilizing wave that threatens to knock us completely into the water.
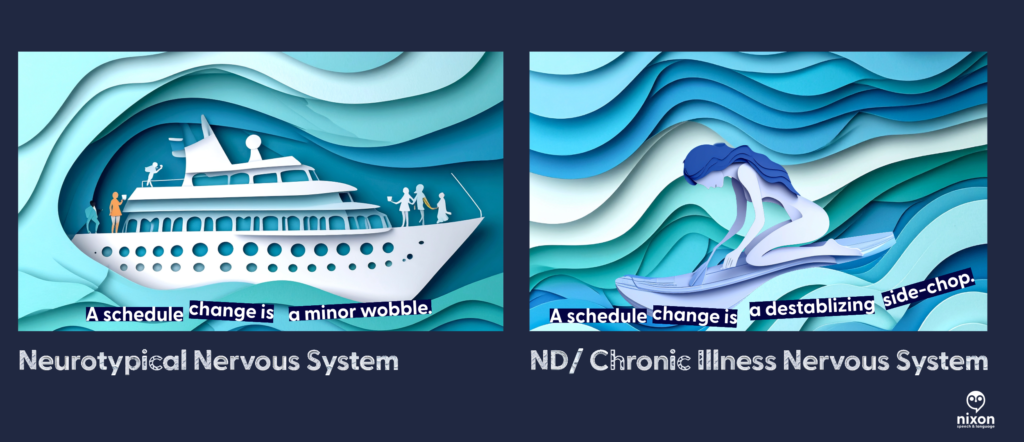
The Metaphor: Most people navigate medical uncertainty on a stable cruise ship. They feel the waves but stay dry. We are on a stand-up paddle board. We require constant, exhaustive internal effort to balance on perfectly calm water. When the system changes, a “ripple” to the cruise ship becomes a catastrophic “tsunami” for us.
The Fatigue: We are exhausted not because we are “weak,” but because we are spending all our energy on a silent, Invisible Brace. Every admin call, sensory input, and physical pain is a wave hitting our wobbly board.
The “Flip”: When we have a meltdown, shutdown, or cancel plans, the “board has flipped.” This isn’t a failure; it’s a necessary, protective reset. We need to “sink” for a minute to stop the adrenaline of trying not to fall.
How to Help: Don’t tell us to “be flexible.” Help us stabilize. Be the solid object we can hold onto. Take over the phone calls and give us the grace to be “underwater” until the sea calms down.
How many of us have heard these words, “Be more flexible”? I didn’t realize that meant my surgery date would be doing yoga while I’m just trying to stay upright. Between the rogue waves of kidney stones and the sinking weight of low ferritin, my medical calendar has become a series of “maybe next weeks” for my lumbar fusion.
To most people, a schedule shift is an inconvenience—a slight tilt on the deck of a cruise ship. But for the neurodivergent and chronically ill, stability isn’t a given; it’s a manually operated system. We aren’t on the cruise ship. We are on a stand-up paddle board in the middle of a high-traffic wake. Each appointment that changes often means changing another appointment, changing a leave request, and navigating yet another unknown.
When the world tells us to “go with the flow,” they don’t see the Invisible Brace. They don’t see the constant, microscopic mental and physical adjustments we make just to keep our heads above the spray. In a medical system that moves like a speedboat, being “flexible” isn’t a personality trait—it’s an expensive, exhausting executive function tax that may eventually lead to our board flipping.
And sometimes, flipping the board is the only way to finally find some peace.
The First Wave
It started with a constant wave pushing my side. A kidney stone—the first rogue wave in a storm I didn’t see coming. Then came the low ferritin, the overwhelming fatigue, and the sudden, sickening realization that my carefully constructed medical plan was no longer a plan; it was a loose suggestion.
In the midst of this chaos, I kept receiving I felt like I just needed to be remain flexible.
But that is a lot to manage: Flexibility is a great trait for a gymnast, but it’s a terrifying requirement for a medical plan. Here is the reality of my recent experience:
The Paddle Board vs. The Cruise Ship
To understand why “going with the flow” is so utterly exhausting for neurodivergent and chronically ill people, you have to understand the difference in our vessels.
Most people experience medical delays or schedule shifts like they are on a massive cruise ship. The floor might tilt, the waves might get choppy, and it’s certainly annoying, but the hull is thick enough to absorb the impact. They stay dry. They stay standing.
But when you are neurodivergent—craving predictability to manage sensory and cognitive loads—or living with chronic illness, you aren’t on a cruise ship. You are on a stand-up paddle board.
Even when the water is perfectly flat, we are already expending significant executive function and physical energy just to maintain balance. Every sensory input, every social interaction, and every administrative task requires a micro-adjustment of our internal stabilization systems.
When the medical boat (the scheduling office, the specialist, the test results) suddenly changes course, it creates a massive wake. For the cruise ship, it’s just more water. For the paddle boarder, it is a catastrophic side-chop that we were not braced for. Telling ourselves to “just stand up” when we have been knocked horizontal by the wake is a misunderstanding of physics.
The Invisible Brace: Taking on Water
If it’s not the main wake from the medical boat, it’s the debris. Being neurodivergent in a medical shift (or even change in what to do next) feels like you are paddling through a constant, exhausting stream of waves you cannot anticipate.
While we are trying to keep our balance, the environment is constantly throwing more waves at us, demanding more “flexibility”:
The Rogue Wave (The Admin Avalanche): Having to make immediate phone calls to rearrange transportation, update employers, or coordinate with multiple specialists, all while processing bad news.
The Side-Chop (Sensory & Cognitive Overload): Navigating an insurance company’s phone menu or reading complex medical instructions while in physical pain and brain fog.
The Undertow (Sensory Dread): Mentally bracing for the specific sensory inputs of an impending procedure, only to have that dread extended indefinitely when the date moves.
This is Tether Fatigue. We are exhausted not because we are “difficult,” but because we have been in a permanent, tense, Invisible Brace for weeks, absorbing the kinetic energy of every ripple. Our energy reserves are fully bankrupted by the sheer volume of waves we’ve had to process just to avoid falling in.
The Grace of the Capsized Board
There comes a point where the balance is lost. The board flips. The paddle boarder goes under. To an observer, this looks like a crisis, a meltdown, or “giving up.”
But here is the secret that the neurotypical world needs to understand: Sometimes, we need to let the board flip.
When we hit the water, the Invisible Brace is finally over. We stop fighting the waves. We stop trying to anticipate the next administrative side-chop. For a moment, there is just the quiet, cold weight of the water.
We aren’t failing to cope; we are allowing the system to reboot because the cost of staying upright on a wobbly board hit by a tsunami has fully bankrupted our energy reserves. We need that “sink time” to stop the adrenaline and let our nervous systems reset before we can even think about climbing back onto the board.
How to Be an Anchor
If someone you love is neurodivergent or chronically ill and their “ship” has just flipped, don’t stand on the shore and yell at them to swim harder. Help them stabilize the water.
Reduce the “Administrative Friction”: When the plan changes, the “to-do” list explodes, requiring executive function we don’t have.
Don’t say: “Let me know if you need anything.”
Do say: “I am standing by a phone. Give me your permission, and I will handle the rescheduling calls today so you don’t have to explain your situation five more times.”
Validate the Physics, Not the Feeling: Don’t gaslight us with positivity. Acknowledge the environment.
Don’t say: “Just keep rowing! Be resilient!”
Do say: “The water is incredibly choppy right now. It makes total sense that you fell. I’m right here when you’re ready to try again.”
Grant the Grace to Sink: Let us stay underwater for a minute. We need that silence to recalibrate before we have the strength to climb back onto the wobbly board.
Examples of Stabilization in Action
Example A: Dear Medical Provider (The View from the Paddle Board)
“When you tell me a surgery is delayed or a result requires a pivot, you might see it as a minor scheduling shift. For my neurodivergent brain and my chronically ill body, it is a tsunami hitting a stationary paddle board. Please help me stay above water:
Reduce the Administrative Friction: Don’t make me the middleman between specialists. Coordinate the update with my other providers so I don’t have to spend my limited energy repeating my trauma five times.
Give Me a Fixed Point: Tell me exactly what the next step is. Ambiguity is a wave I cannot balance on.
Example B: Dear Friend (When My Board Flips)
“Right now, the floor is shaking. I am exhausted from trying to ‘stay upright’ on a board that feels every single ripple. When you see me overwhelmed, please know that I’m not being difficult—I’m bankrupt from navigating a constant stream of administrative and sensory cross-currents. Here is how to be my anchor:
Don’t Ask, Just Do: Telling me ‘I’m bringing over safe food at 6:00 PM’ is infinitely more helpful than ‘Let me know what you need.’
Let Me Sink: If I cancel, don’t take it personally. My board has flipped, and I promise I’ll climb back on when the sea calms down.”
Flexibility isn’t a personality trait; it’s an expensive resource. For the neurodivergent and chronically ill, “going with the flow” often means fighting the current just to avoid drowning. Sometimes, the best way to help us is to just let us float until the sea is still again.
Note about the art:
To capture the “layered” nature of neurodivergent life, I used a collaborative AI process to create the visuals for this post. I worked with Adobe Firefly to generate the base “paper-cut” style and used Gemini as an “Art Director” to refine the metaphors—ensuring the “administrative debris” and the “underwater reset” felt as visceral as the words themselves.
With a unique perspective shaped by my own learning disabilities, including ADHD, I bring a wealth of professional expertise in education and health policy, grant review, as well as research, evaluation, and treatment of children with speech, language, and reading disorders.
My passion lies in advocating for those who are not able to do so for themselves, leveraging my diverse background – both personally and professionally – to make a meaningful impact in the field of special education and child development.


 medical gaslighting and the importance of accurate, data-driven medical records for neurodivergent (AuDHD) patients." class="wp-image-967" srcset="https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-1024x1003.png 1024w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-300x294.png 300w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-768x752.png 768w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-1536x1505.png 1536w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-2048x2006.png 2048w" sizes="(max-width: 1024px) 100vw, 1024px" />
medical gaslighting and the importance of accurate, data-driven medical records for neurodivergent (AuDHD) patients." class="wp-image-967" srcset="https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-1024x1003.png 1024w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-300x294.png 300w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-768x752.png 768w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-1536x1505.png 1536w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-2048x2006.png 2048w" sizes="(max-width: 1024px) 100vw, 1024px" />



Leave a Reply neurodivergence/#respond" style="display:none;">Cancel reply