
Words have Weight: The Mirror Test, Part 1b
Provider Track: Would you want these words in your permanent record?
Disclaimers.
Professional Standards and Scope:
- Credentials and expertise: Dr. Stephanie Michelle Nixon is a PhD-level Speech-Language Pathologist and consultant.
- Educational purpose: The content in this series is shared for informational, educational, and advocacy purposes only.
- No clinical relationship: Engagement with this content does not constitute medical advice, a clinical diagnosis, or the establishment of a patient-provider relationship.
- Medical consultation: Always seek the advice of your physician or other qualified health providers with questions regarding a medical condition.
Personal Narrative & Data Integrity:
- Designated Record Set: This series represents a personal, professional audit of my own legally obtained medical history and “Designated Record Set”.
- Factual Basis: All clinical data points—including the 169.4-minute gastric emptying result —are pulled directly from my documented clinical records.
- Advocacy Intent: My goal is to highlight systemic disparities in medical documentation and foster better clinical communication.
- Non-Defamation: This audit is a critique of the content and quality of documentation and the patterns of clinical bias, rather than an attack on specific individuals or institutions.
A Note on Neurodivergent Baseline:
Contextual Accuracy: Observations regarding communication style, energy, or behavior (often labeled “manic” or “pressured” in my records) must be viewed through the lens of my documented, lifelong ADHD diagnosis.
A ‘u’ was added (AuDHD) as a late diagnosis a few years ago providing a key to understanding why so many providers saw ‘manic’ behavior where there was actually just a neurodivergent person managing a health emergency. We have to stop labeling what we don’t understand.
 medical gaslighting and the importance of accurate, data-driven medical records for neurodivergent (AuDHD) patients." class="wp-image-967" srcset="https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-1024x1003.png 1024w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-300x294.png 300w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-768x752.png 768w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-1536x1505.png 1536w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-2048x2006.png 2048w" sizes="(max-width: 1024px) 100vw, 1024px" />
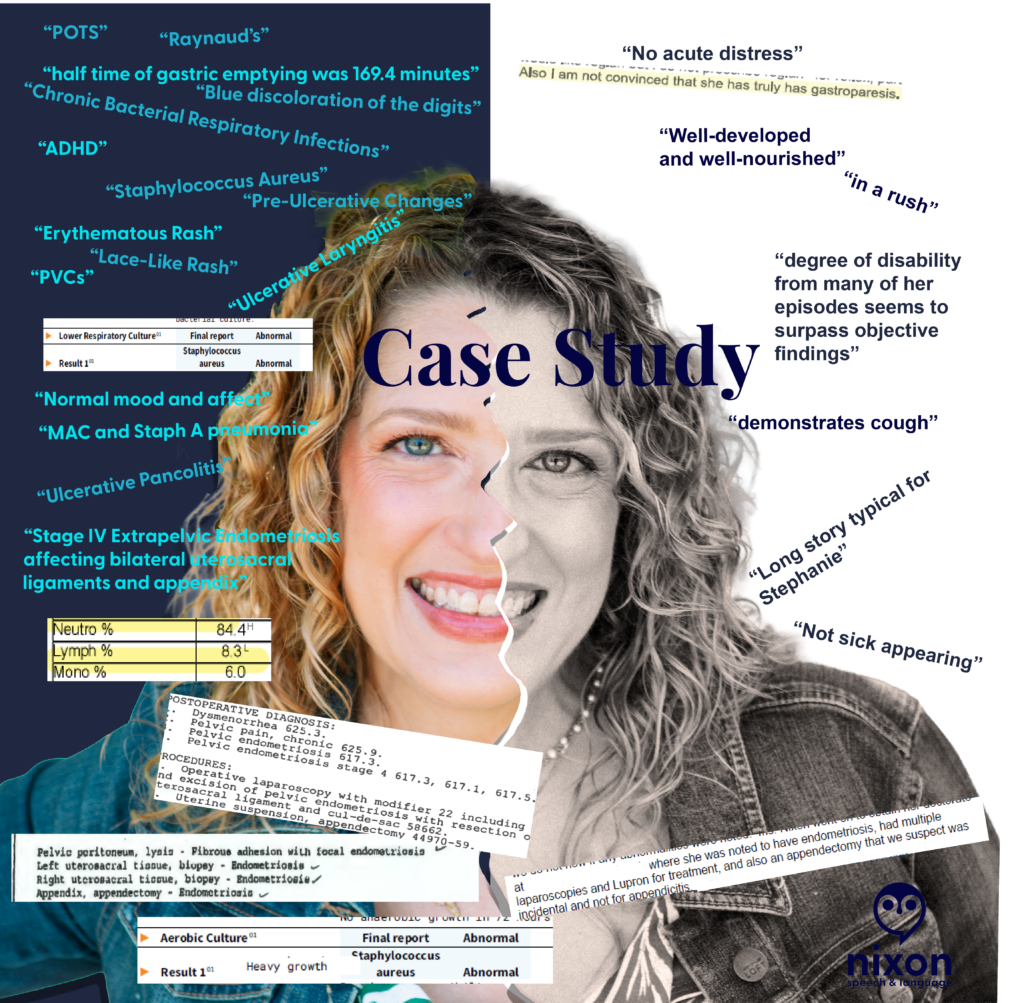
medical gaslighting and the importance of accurate, data-driven medical records for neurodivergent (AuDHD) patients." class="wp-image-967" srcset="https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-1024x1003.png 1024w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-300x294.png 300w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-768x752.png 768w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-1536x1505.png 1536w, https://nixonspeechandlanguage.com/wp-content/uploads/2026/05/Case-Study-Bias-in-chart-notes-2048x2006.png 2048w" sizes="(max-width: 1024px) 100vw, 1024px" />Clinical documentation is a record of pathology, not a character assessment. Yet, after auditing my own medical records, I found decades of “subjective” notes that had nothing to do with my physiological state and everything to do with a provider’s snap judgement and dismissal of my lived reality.
It doesn’t matter if a provider feels these words “justified” in the moment. Once they are in the patient’s chart, they become a permanent filter for every provider who follows.
The words on the black and white side minimize and dismiss both objective findings and my symptoms.
In the image above, a provider documented that my degree of disability ‘surpassed objective findings.’ In doing so, they failed to recognize my functional reality: I was a Speech-Language Pathologist unable to see my patients for 3 weeks after losing my voice to an ulceration on my vocal fold. When documentation focuses on ‘surpassing findings’ but ignores a total loss of vocational function, the clinical record is incomplete. We must document the patient’s life, not just the provider’s impression.
The Scope-of-Practice Gap:
I found repeated psychiatric judgments—labels like ‘pressured speech’ and ‘somatization’—written by specialists who were not psychiatrists or behavioral neurologists. Labeling a communication style as ‘pressured speech’ without establishing a neuro-informed baseline (AuDHD) isn’t just a misinterpretation—it is a specialist overstepping their scope to pathologize a natural speech rate instead of investigating physical health.
What they called “pressured”:
- A Neurodivergent Baseline: If anyone had paused to ask, I would have laughed and told them that I had the words “SLOW DOWN!” in bold on every note for every presentation during my post-graduate education.
- Physiological Distress: Rapid speech and “short rushes” are frequently associated with shortness of breath. Documentation that reaches for a psychiatric label while a patient is in respiratory distress is a failure of clinical reasoning.
- Fluency Dynamics: As an SLP, I recognize these patterns as potential symptoms of cluttering among other speech and language disorders.
None of these clinical presentations require a mental health diagnosis. When we reach for mental health labels to describe a fast speech rate, we ignore the very real physical or fluency-based realities of the patient standing in front of us.
The “Incidental” Dismissal
I once had a specialist (not a gynecologist or GI) dismiss my appendectomy as “incidental” to my laparoscopy for Stage IV extra-pelvic endometriosis. When a pathology report confirms ‘Appendix – Endometriosis,’ that appendectomy is a diagnostic data point, not an ‘incidental’ event. Labeling it as such signals to every future provider that the patient’s surgical history—and their reported pain—is irrelevant.
The Receipts:
- The Science: A 169.4-minute gastric half-time (normal is <90) was dismissed by a specialist who was “not convinced.”
- The Paradox: A 65% O2 saturation reading was recorded alongside a note that I was “well-appearing”. (Note. The 65% O2 reading was likely associated with PVCs based on the other data in the visit.)
- The Shorthand: A systemic crisis involving a 20-lb weight gain and pitting edema was labeled “long story typical for Stephanie”.
The Challenge:
- The Mirror Test: If you were the patient, would you want a crisis described as “typical” for you?
- Stay in Scope: If you aren’t a psychiatrist, why are you reaching for psychiatric labels to describe a patient’s communication? (Also, check with the patient. Had that provider asked me, I would’ve laughed and told her that my rate of speech has always been fast…in fact, I must actively think about it to speak more slowly.)
- Watch for Bias: Literally watch for it. If you see a dismissive note from a colleague, don’t carry it forward. Check the data, ask the patient, and document the objective truth.
Let’s hold the record to a higher standard. How can we ensure our “Subjective” notes don’t do lasting harm?
Access and advocacy, chronic illness, clinical documentation bias, empower patients, invisible illness, more than labs, neurodivergence, patient advocacy in healthcare, subjective vs. objective medical notes
Leave a Reply