
Words Have Weight: The “Saga” of Subjective Charting
Part 2B: Provider Track – Liability of the Filter
Personal Narrative & Data Integrity:
- Designated Record Set: This series represents a personal, professional audit of my own legally obtained medical history and “Designated Record Set”.
- Factual Basis: All clinical data points—including the 169.4-minute gastric emptying result —are pulled directly from my documented clinical records.
- Advocacy Intent: My goal is to highlight systemic disparities in medical documentation and foster better clinical communication.
- Non-Defamation: This audit is a critique of the content and quality of documentation and the patterns of clinical bias, rather than an attack on specific individuals or institutions.
A Note on Neurodivergent Baseline:
Contextual Accuracy: Observations regarding communication style, energy, or behavior (often labeled “manic” or “pressured” in my records) must be viewed through the lens of my documented, lifelong ADHD diagnosis.
A ‘u’ was added (AuDHD) as a late diagnosis a few years ago providing a key to understanding why so many providers saw ‘manic’ behavior where there was actually just a neurodivergent person managing a health emergency. We have to stop labeling what we don’t understand.
Clinical documentation is a legal and clinical record. It should describe findings, reasoning, function, and uncertainty—not turn subjective impressions into a durable patient identity.
When providers prioritize narrative shorthand over objective data, the consequences extend beyond patient frustration. Subjective charting can bias future providers, delay appropriate workup, and create significant medicolegal risk.
The Choice: A Thread or a Relationship?
In a research study by Melanie Sloan and colleagues¹, one patient described her medical record as:
“A deranged Twitter feed… creating a completely unrecognizable image of me as a patient and a person.”²
As a provider, you have a choice:
- The “Deranged Twitter Feed”: Do you want to be just another reactionary post in a chaotic thread of subjective dismissals?
- The Anchor of Trust: Or do you want to be the provider they respect—the one who actually listens and anchors the record in data?
If you entered medicine for an ego trip or to exert power, there is no point in reading further. But if you are here to help, then I am asking you—as both a provider and a patient—to LISTEN.
The Contrast: Storytelling vs. Clinical Data
When you read a previous provider’s note describing a complex illness as a “saga,” it creates a powerful cognitive bias. It can cause you to actively ignore objective data sitting right in the chart.
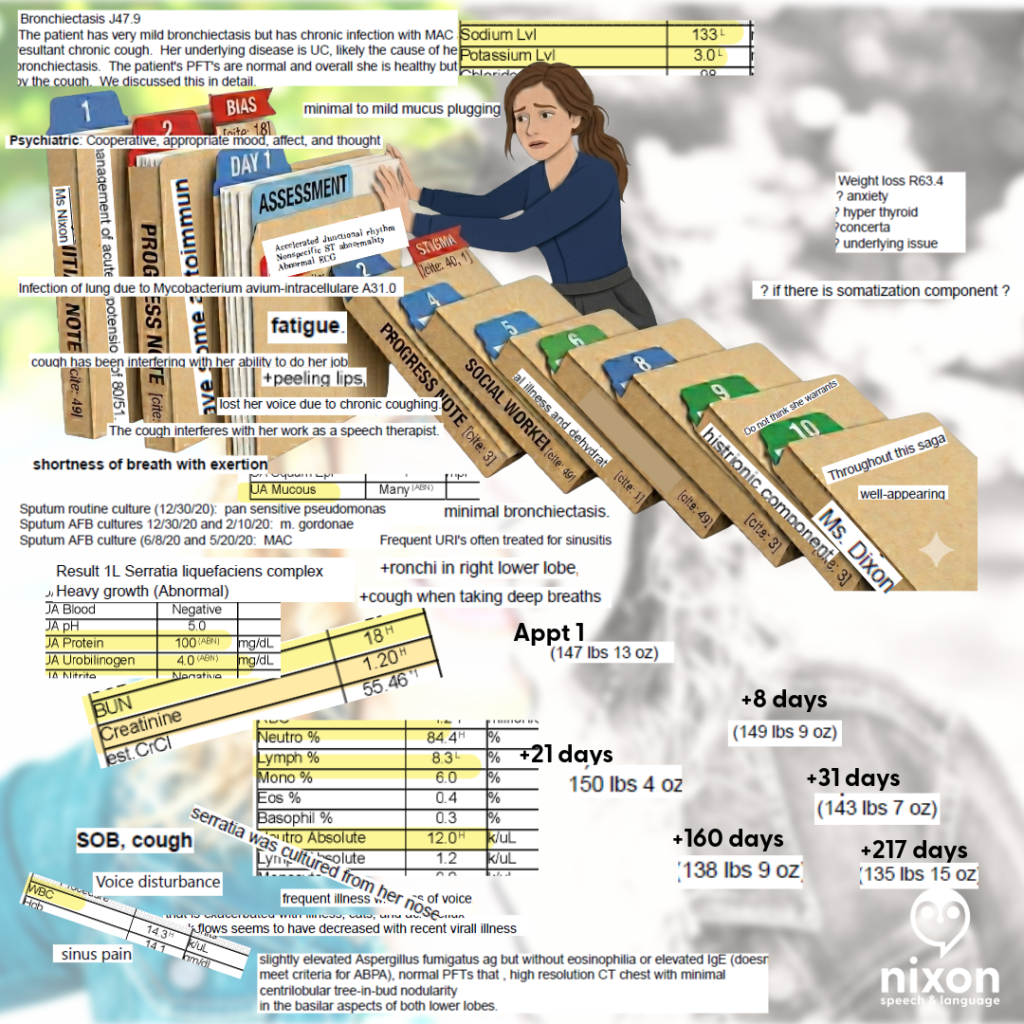
Case Study: The “Histrionic” Filter vs. The Objective Truth
Consider one of my ER visits. Likely primed by a previous provider’s “saga” label, the clinician documented: “There is a histrionic component to her presentation.”
What the clinician ignored to maintain their narrative:
- Hypovolemic Shock: My blood pressure was 80/51, requiring 39 minutes of critical care.
- Inflammatory Markers: A WBC of 14.3, Neutrophils: 84.4%, Lymphocytes: 8.3%.
- Radiographic Evidence: A High-Resolution Chest CT finalized one week prior explicitly documented “tree-in-bud nodularity,” the radiographic hallmark of small airway mucus plugging and infection.
When you allow a biased adjective to anchor your judgment, you write a psychiatric label on a patient whose complaint is legitimate and objectively noted in labs and imaging. And you become another domino falling in the chain all because you didn’t review all the data or allowed your diagnosis and assumptions to be guided by others. This is an indefensible medicolegal liability.
Clinician Associated Trauma (CAT) is Real
Clinician Associated Trauma is the cumulative psychological harm caused by repeated medical gaslighting and biased charting.
- The “Organization” Trap: I provided a chronological timeline of my worsening cough in hopes they would understand, only to have it called a saga. I spent the past 5 years trying to better organize my history, only to have it referred to as “30 pages of notes”.
- The Identity Error: When Precision Fails
In January 2020, a resident referred to my three-month medical crisis as a “saga” while incorrectly identifying me as “Ms. Dixon”. Most notably, the attending physician then signed off on this report, attesting that they “reviewed the resident’s note and agree with the history” .
In educational settings, using the wrong name on a child’s report would likely render the document invalid. In medicine, however, we allow a senior clinical supervisor to “verify” an error-ridden note, giving subjective character assessments the weight of permanent clinical truth. If a provider isn’t precise enough to get your name right, they aren’t precise enough to label your experience.
- The “Rubber Stamp” Risk: When you sign an attestation for a note containing an incorrect patient name or biased labels like “saga,” you are professionally validating a “deranged twitter feed” entry.
- The Transparency Reality: Under the 21st Century Cures Act, patients see your attestation immediately. If you are too rushed to catch a wrong name, the patient (and the law) will assume you were too rushed to perform a rigorous clinical review.
- The Clinical Standard: If a document’s basic identifiers are wrong, its clinical conclusions are suspect. Use your edit window to ensure the final record reflects the objective truth, not a “rubber-stamped” narrative.
Technical Stewardship: Closing the Gap
Longitudinal aggregation is the best defense against fragmented care.
- Guava Health: Allows providers to reconcile conflicting documentation and see the “receipts”—like a 169.4-minute gastric half-time—before a subjective bias can take root.
- Google Workspace + BAA: Provides secure, HIPAA-compliant infrastructure to handle high-stakes documentation.
The Correction as a Collaboration
Under the 21st Century Cures Act, the wall between the patient and the record has been removed. If an error exists, they will see it.
- Acknowledge the Discrepancy: Respond with empathy: “I am sorry there are discrepancies… I am on your side!”, but mean it.
- Avoid Blaming the Patient: Even if the patient had a chance to review whatever the documentation, it isn’t their fault the chart is wrong. That’s the provider’s job.
- Update the Record: Whether through an addendum or voiding a note, ensure the final record reflects the functional and physiological truth.
Humanity Over Perfection: The Due Diligence Standard
We are all human. Patients don’t expect their providers to be perfect; they expect them to do their due diligence .
Mistakes happen—a wrong name, a misinterpreted symptom, a “rubber-stamped” attestation . But the difference between a “mistake” and “Clinician Associated Trauma” is the willingness to be honest when your own “spoons” (capacity/energy) are lacking.
The “Honest Pivot” Script
If you are overwhelmed, behind schedule, or hit a wall with a complex case, don’t reach for a “saga” label to end the visit. Try radical honesty instead:
“I want to be fully present for this conversation, and I know you took the time to come in today. Honestly, my capacity is low right now, and I want to give your data the deep thought it deserves. Can I review your records this week and follow up with a call or a telehealth visit in 10 days to discuss my findings?”
Why This Pivot Saves the Relationship:
- It Models Respect: You are acknowledging that the patient’s time and data are valuable.
- It Prevents Bias: By pausing instead of rushing, you avoid making the “snap judgments” that lead to “histrionic” labels or identity errors.
- It Shifts the Dynamic: You are no longer the “gatekeeper” with all the answers; you are a partner performing an audit.
The Provider Challenge: The Mirror Test
- Stay in Scope: If you are not a psychiatrist, do not reach for labels like “pressured speech” to pathologize a communication style. Investigate neuro-informed baselines (AuDHD) or physiological distress first. As I said in Part 1 – there are many reasons a person might speak with a fast rate beyond anxiety (and they aren’t zebra reasons…).
- Document Uncertainty, Not Assumptions: Do not use psychiatric labels as a “wastebasket” for difficult diagnostics. Similarly, ask yourself … why is this patient bringing 30 pages of “hand-typed notes” to my appointment?
Sometimes…the answer is as simple as the patient doesn’t want to forget the name of the 12 medications or…the patient’s hand cramps writing on your background history forms, so they have it available to print for providers. And other times…their history is just that long.
Don’t assume their physical symptoms are anxiety – some of us blank when people ask questions, that doesn’t mean it’s somatization or anxiety.
- Audit Your Adjectives: Adjectives that frame symptoms as a performance (“claims,” “dramatic,” “demonstrates”) transmit bias to every clinician who follows.
- Document Function, Not Assumptions: I was an SLP unable to work for 3 weeks due to a vocal fold ulceration, yet a provider wrote my disability “surpassed objective findings”. Document the loss of function, not your “impression
The Bottom Line: Be the Partner, Not the Domino
A corrected chart or a thoughtful follow-up isn’t a sign of weakness; it is a higher standard of Clinical Data Stewardship. It protects you from medicolegal liability and ensures that every future provider sees a clear, objective physiological truth—not a “deranged twitter feed” of biased shorthand.
If you became a provider because you want to help, then be the one who keeps the dominos standing.
Bottom Line: A corrected chart isn’t just a win for the patient; it is a higher standard of Clinical Data Stewardship that protects you and ensures every future provider sees the truth, not a “saga”.
References
- Sloan, M., Naughton, F., Harwood, R., Lever, E., D’Cruz, D., Sutton, S., Walia, C., Howard, P., & Gordon, C. (2020). Is it me? The impact of patient-physician interactions on lupus patients’ psychological well-being, cognition and health-care-seeking behaviour. Rheumatology Advances in Practice, 4(2), rkaa037. https://doi.org/10.1093/rap/rkaa037
- Sloan, M., Bosley, M., Gordon, C., et al. (2025). “‘I still can’t forget those words’: mixed methods study of the persisting impact on patients reporting psychosomatic and psychiatric misdiagnoses.” Rheumatology. doi: 10.1093/rheumatology/keaf115. PMID: 40037287; PMCID: PMC12107051.
- Davis, B. (2021). “Derogatory Language in Charting: The Domino Effect.” Patient Safety Network. https://patientsafetyj.com/article/73542-derogatory-language-in-charting-the-domino-effect
- Goddu, A. P., O’Conor, K. J., Lanzkron, S., et al. (2018). “Do Words Matter? Stigmatizing Language and the Transmission of Bias in the Medical Record.” Journal of General Internal Medicine, 33(5), 685–691. doi: 10.1007/s11606-018-4583-7. PMID: 29374357; PMCID: PMC5910343.
- Park, J., Saha, S., Chee, B., Taylor, J., & Beach, M. C. (2021). “Physician Use of Stigmatizing Language in Patient Medical Records.” JAMA Network Open, 4(7), e2117052. doi:10.1001/jamanetworkopen.2021.17052
- Barcelona, V., Scharp, D., Idnay, B. R., et al. (2024). “Identifying stigmatizing language in clinical documentation: A scoping review of emerging literature.” PLOS ONE, 19(6). doi: 10.1371/journal.pone.0303653. PMID: 38941299; PMCID: PMC11213326
- Silverman, K. (2023). “Improving Health Equity by Eliminating Biased and Stigmatizing Language in Medical Notes.” Center for Health Care Strategies.
- CRICO (2021). “Cures Act Overview”. https://www.rmf.harvard.edu/Risk-Prevention-and-Education/Article-Catalog-Page/Articles/2021/Cures-Act-Overview
- Pandita, D., Johnson, D., & Bledsoe, T. A. “Lab Results Reporting, Ethics, and the 21st Century Cures Act Rule on Information Blocking.” ACP Ethics Case Study Series. https://www.acponline.org/clinical-information/medical-ethics-and-professionalism/ethics-case-studies-education-resources/lab-results-reporting-ethics-and-the-21st-century-cures-act-rule-on-information-blocking
- HHS.gov (2025). Your Medical Records: https://www.hhs.gov/hipaa/for-individuals/medical-records/index.html
- Google Workspace (2026). “Gemini for Workspace: Enterprise Privacy and Model Training Standards.” https://knowledge.workspace.google.com/admin/gemini/generative-ai-in-google-workspace-privacy-hub
- TeamAI (2026). https://teamai.com/blog/large-language-models-llms/gemini-models-explained-the-complete-2026-guide/
For more information about Guava Health go to https://guavahealth.com/ For more information about the FitBit transformation to Google Health coming 5/19/2026 go to https://health.google/
Access and advocacy, chronic illness, clinical documentation bias, Clinician Associated Patient Trauma, medicolegal risk, patient advocacy in healthcare, patient gaslightling, providers