Google Health’s: The Master of Context and Your Early Warning System
Please review my blog disclaimers and disclosures
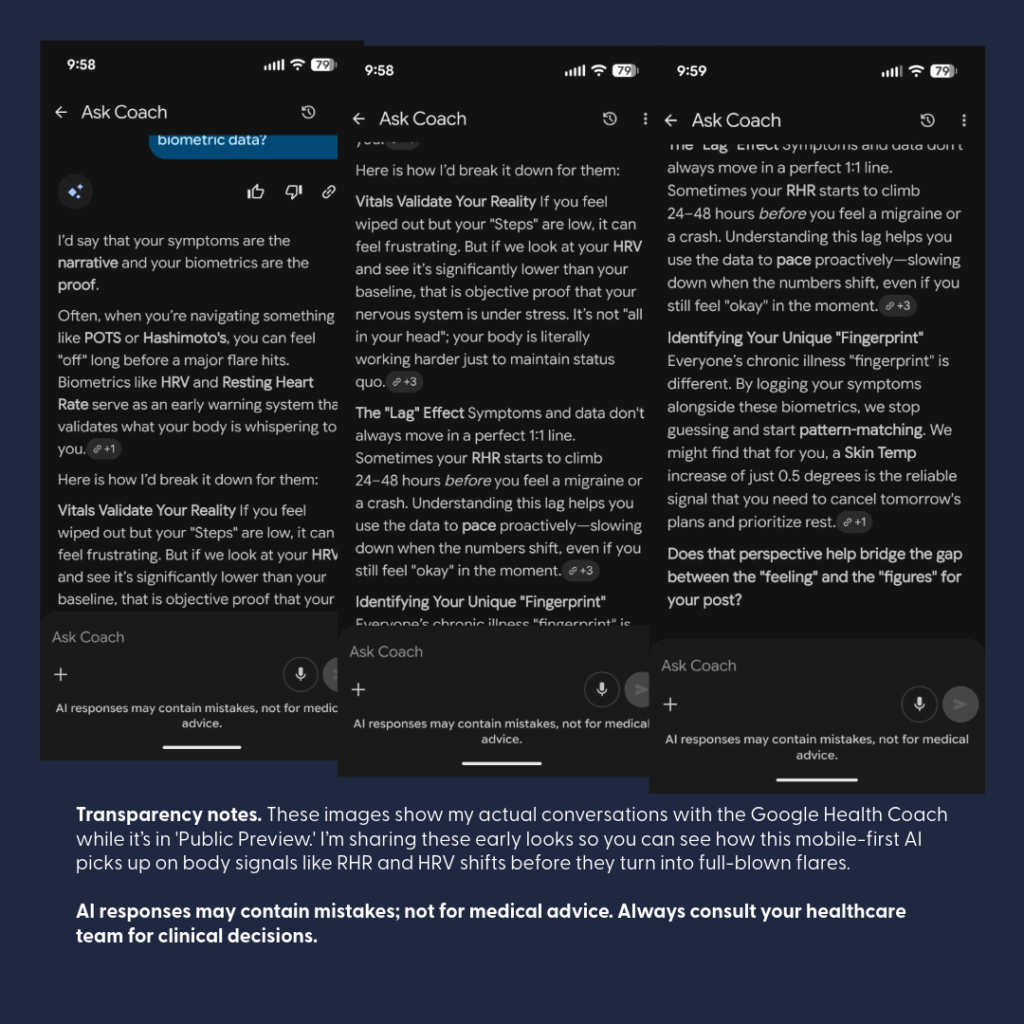
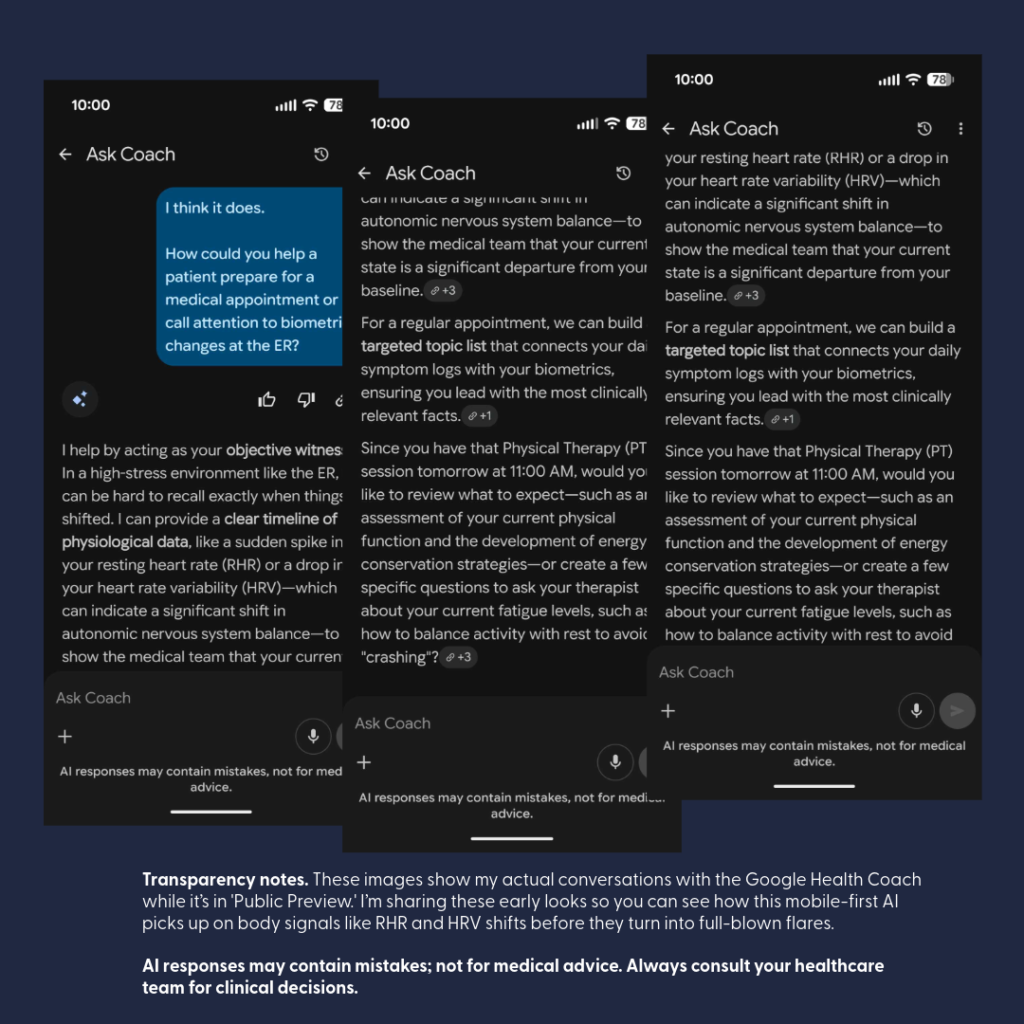
Transparency & Context: My Beta Experience
- Note on Personalization: Screenshots are from my real-world testing of the Google Health (formerly Fitbit) “Coach” during its beta rollout. These represent a highly personalized conversation. Because I have been “talking” with Gemini for a long time (in Google and in FitBit Pro), the AI has a longitudinal understanding of my specific medical roadmap—including things like my C5-7 disc replacement and chronic pacing goals.
- No Guarantee of Results: Each user may have a different initial experience or conversation flow. Like any “learning partner,” the depth of the insights often depends on the context you provide over time.
- Beta & Evolving Features: These visuals are part of the Fitbit Labs “Public Preview”. Features like “Unusual Trends” detection are currently in testing and may change or evolve over time.
- Standard Safety Reminder: AI responses may contain mistakes and are not for medical advice. Always consult your healthcare team for clinical decisions.
Let’s talk about the Google Health Rollout that began May 19, 2026! I have been participating in the beta for FitBit Pro users, and I must say, I am impressed!
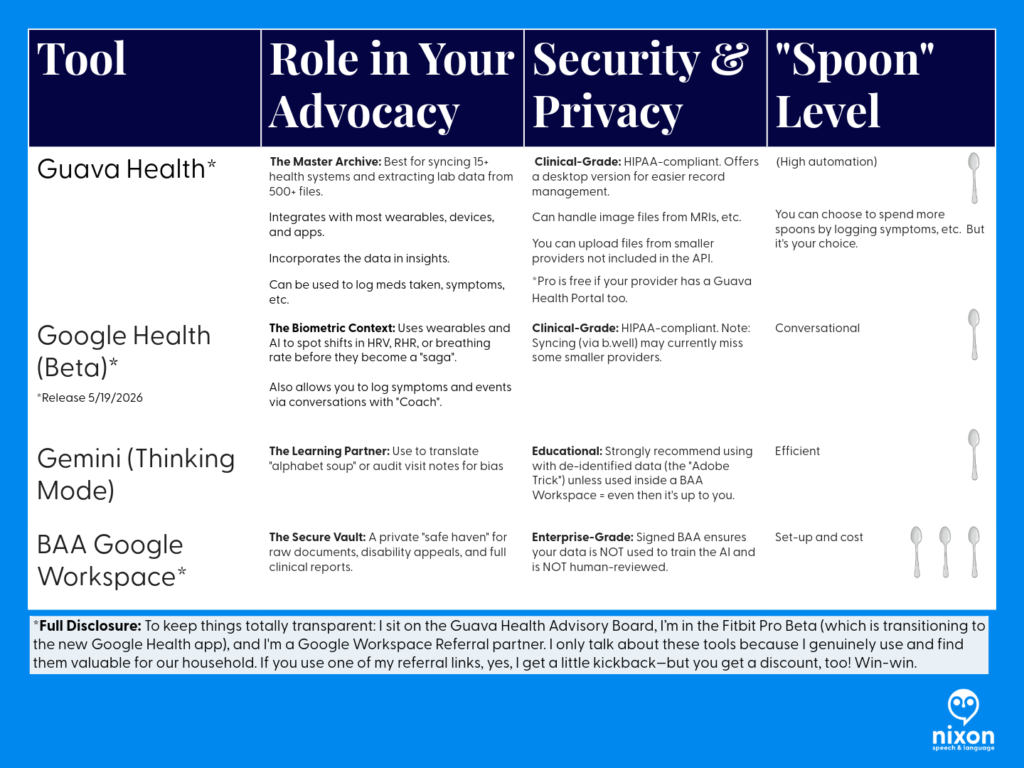
(It won’t replace Guava Health for me, but it is a wonderful addition.)
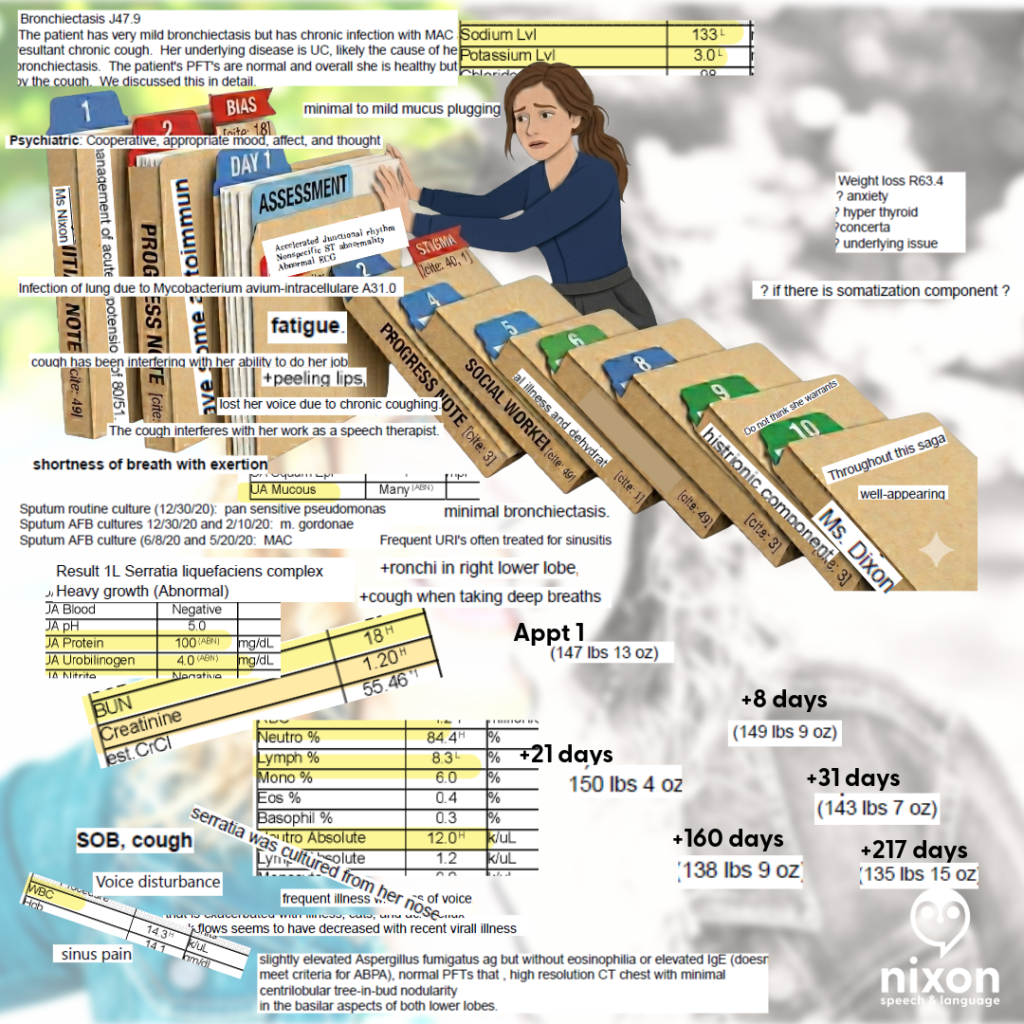
Have you ever walked into a follow-up appointment, described a new and terrifying symptom, only to be told it’s “just part of the healing process” or “normal”? When a provider dismisses your symptoms, they are often guessing and comparing your body to a textbook average. To get them to move from guessing to investigating, you need objective data.
TANGENT: If you find this interesting, check out the Words have Weight Series that I’m posting!
Walking into a clinic with your biometric data (including trends noted by your wearables) helps to change the dynamic: you are comparing you to YOU. Turning personal data into clinical leverage is the ultimate evolution of patient advocacy.
Google Health’s major platform rollout gives patients with chronic conditions a new set of tools to add to their baseline strategy. Here are some ways you can use this rollout to audit your care and bring the facts to your next appointment.
Master of Context and an Early Warning System
The new Google Health platform brings a clinical-grade environment directly to your phone. Google Health Premium (formerly FitBit Health Pro) serves as the home for the platform’s full Health Coach features.
Google Health is designed specifically to be the Master of Context. The mobile AI “Coach” can provide an “Early Warning System” for your day-to-day well-being:
- The Coach is built to “talk” directly to you, your live wearable data, tracking key metrics like Heart Rate Variability (HRV), Resting Heart Rate (RHR), and Breathing Rate.
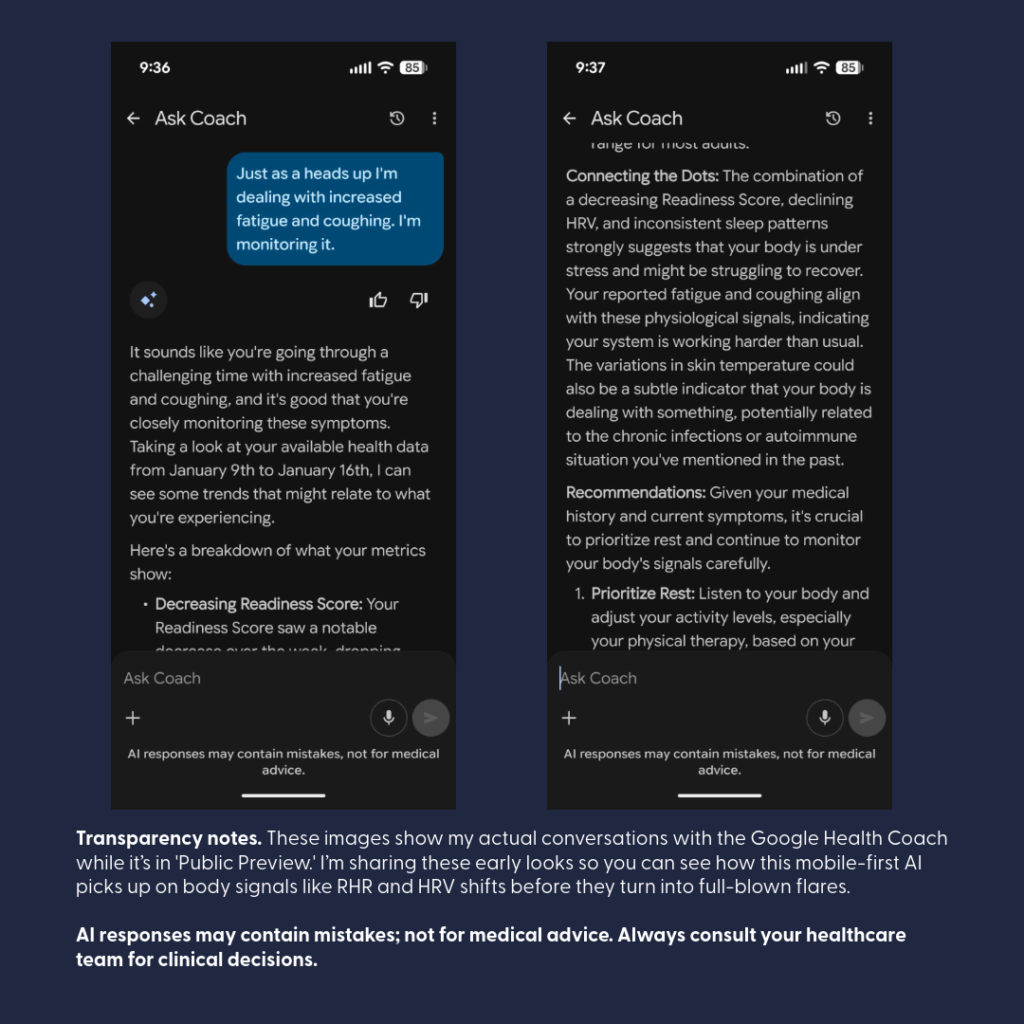
- By continuously analyzing these metrics, the AI can pick up on subtle physiological shifts before you even consciously feel sick, helping you spot trends.
- The conversational interface makes it excellent for quick, on-the-go checks to evaluate the potential impacts of medications, treatments, or even review that “something is off with my body” feeling.

The AI Coach in Google Health can take those raw metrics a step further: it can actively recognize the metrics outside YOUR normal (e.g., resting heart rate increase). Increased resting HR can be associated with autonomic imbalance (Borhani et al., 2025), illness (Michard & Saugel, 2025), and as a key metric for remote arrhythmia management (Jena et al., 2025).
In my case, “Coach” recognized something was off as shown above – and what was off – well I had a kidney stone occluding the lower pole of a ureter. (Complete duplication of my ureters bilaterally … is interesting.)
When undergoing back-to-back iron infusions, the Coach can catch delayed shifts in your biometric data indicating an “adverse reaction” to a medication (i.e., Your body and the medication – didn’t get along).
Having that data readily available allows you to make safe, immediate adjustments with your care team to swap out the problematic medication before your next round, while the Coach continues chatting through your follow-up to monitor your recovery trajectory.
Externalizing Medical Memory
When you’re dealing with chronic illness or a sudden flare, your brain is already working overtime just to handle the pain and exhaustion. Expecting yourself to remember every single detail about when a symptom started or how your heart rate shifted is like trying to run a marathon while carrying a heavy suitcase.
Using a tool like Google Health isn’t about being ‘anxious’—it’s about being smart. It’s like having a backup drive for your brain. You let the app handle the heavy lifting of storing the data so you can save your limited energy—your ‘spoons’—for actually getting through the day and focusing on your recovery.
Offloading data recall to Coach can help you save your energy for the actual clinical conversation. This can help you present objective shifts in your objective data (i.e., biometrics).

The Gemini integration inside the Google Health Coach changes how you interact with your health metrics. Instead scrolling through a list, the Coach synthesizes complex data into clear, plain-language summaries. This can be a relief for patients who feel completely overwhelmed by the “alphabet soup” of data during a physical flare.
Conversational Symptom Logging
As a Guava Health User, I am used to a symptom-tracking checklist that leads to “insights” paired with biometric data. So switching to indirect symptom logs that came out of my conversations with the AI Coach was initially uncomfortable to me.
If you want a rigid, heavily itemized manual symptom-tracking checklist, Google Health’s baseline menus leave a bit to be desired. There is an “other” section, but it isn’t extensive, and it won’t replace the deep, structured manual entry interfaces found in heavy lifters like Guava.
But here is the magic: it completely flips the script by tracking your symptoms through fluid conversation instead. The Coach is incredibly aware of your specific, ongoing body context—for instance, it remembers and keeps tabs on a stubborn ankle injury. Instead of forcing you to click through endless checkboxes and dropdown menus when you are low on “spoons,” you simply talk to the Coach about how you are feeling, and it handles the tracking dynamically within your chat history.
The Longitudinal Brain: Memory Across Threads
Traditional AI tools often suffer from “amnesia,” resetting entirely every time you open a new window. Because Google Health Coach archives core context into persistent memory logs, it builds an ongoing longitudinal understanding of your medical roadmap.
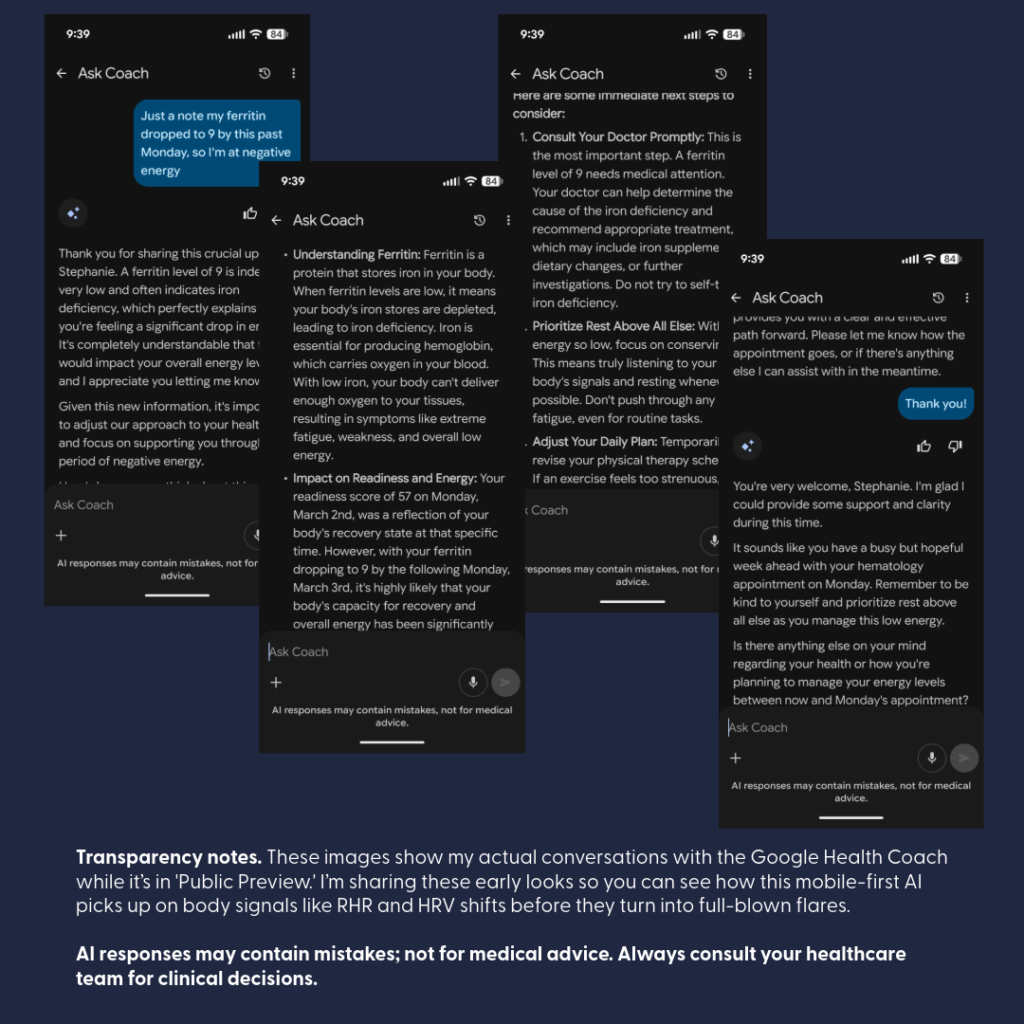
For example, if you discuss a scheduled spinal fusion that gets pushed back due to sudden low Ferritin, the Coach remembers that timeline.
Weeks later, when you open an entirely separate chat session to ask about an isolated biomarker, the AI doesn’t start from scratch—it remembers your overarching journey, bridges the gap between different conversation loops, and actively checks back in on how you’re feeling ahead of the rescheduled surgery. It behaves like a true, long-term cognitive partner rather than a temporary chatbot.
Strict Privacy Guardrails & Clinical Security
Moving your health metrics into a consumer app understandably raises questions about data security. To address this, Google has implemented rigorous technical, administrative, and physical safeguards to ensure this environment meets strict HIPAA (Health Insurance Portability and Accountability Act) standards for storing and transmitting medical records.
Here are the strict guardrails established for the Google Health app rollout:
- Complete Data Separation: Your clinical and wearable health profiles are kept in strict privacy silos, entirely separated from other consumer services like your Google Search history or YouTube recommendations.
- No Ad Targeting or Data Selling: Google has committed to a strict guardrail: your personal health records, diagnoses, and daily biometric data are never sold to third parties and will never be used to target Google Ads.
- Legal Accountability (BAAs): Google Cloud and its health services support compliance through formal Business Associate Agreements (BAAs)—formal contracts that hold the platform legally accountable for protecting your private health information.
- Total Patient Control: You retain full ownership of your profile. You choose exactly which health portals to connect, and you have the power to revoke that access at any moment.
- Granular Location Protections: For privacy-conscious or neurodivergent users, GPS tracking is strictly opt-in. Location data is primarily used to track distance and pace for specific outdoor activities, and permissions can be disabled at any device or app level at any time.
- De-Identified Research: Participating in health research is completely voluntary and never automatic. Before any data is utilized, it undergoes strict de-identification protocols to remove personal identifiers (like names or emails) and is aggregated with data from thousands of others to study broad public health trends.
The “Spoon-Level” Google Health Strategy
When your energy is limited, preparing for a medical visit shouldn’t waste your precious “spoons”. You can easily adapt your use of Google Health to match your capacity on the day of your appointment:
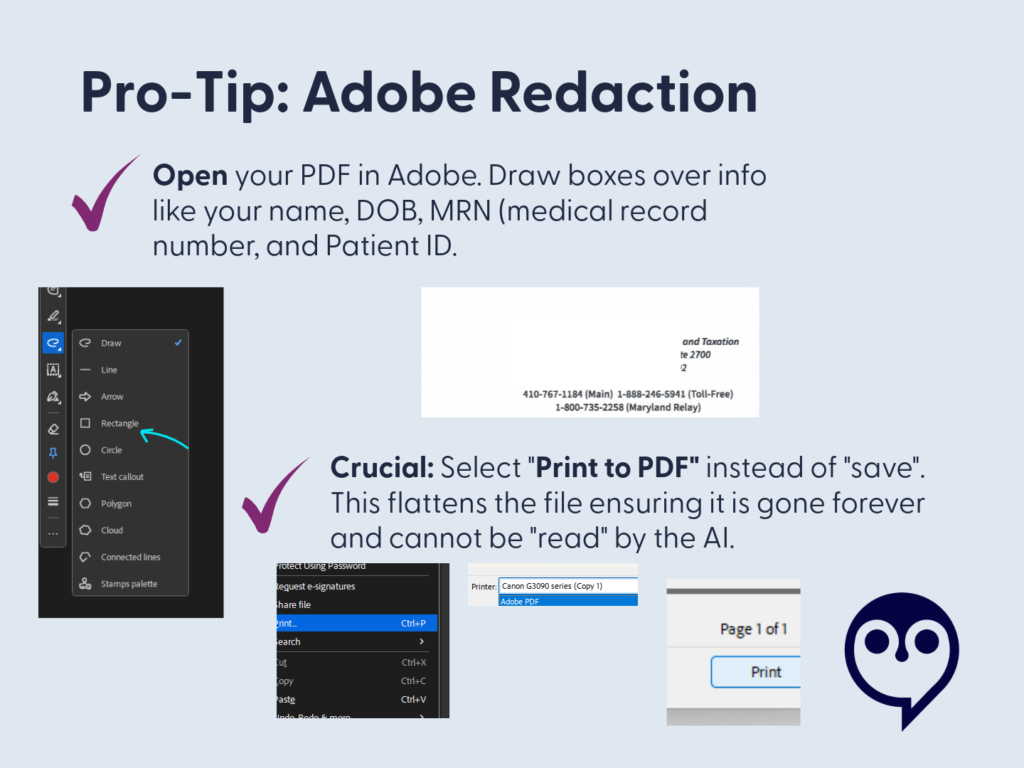
- The Medium-Energy Strategy (🥄🥄): Open your mobile app and ask the Google Health Coach to generate a summary of your recent biometric shifts.
- The Outcome: Print out the AI-generated summary to serve as an instant, objective “talking points” script. This ensures your most critical concerns are accurately addressed even if you hit a wall of brain fog or pain in the exam room.
The Bottom Line
Using an app to monitor your physiological baselines and symptom clusters isn’t a temporary tech trend—it is a necessary act of accessibility for patients navigating complex conditions.
You are not “obsessing” over your health; you are actively partnering in your care.
Utilizing these clinical-grade tools ensures that your medical chart reflects your true physical reality, forcing providers to move past standard labels and look directly at the facts.
Disclaimer: This post is for educational and patient advocacy purposes only. All product names, logos, and brands are property of their respective owners. “Google Health” and “Fitbit” are trademarks of their respective holders. Use of them does not imply any affiliation with, endorsement by, or sponsorship by them.
Citations
Access and advocacy, AI for health, chronic illness, google health, patient advocacy in healthcare, wearable technology