
Stephanie M. Nixon
Experienced Speech and Language Consultant in the Washington D.C., Maryland, Virginia (DMV) metro area.
When the board flips: Paddle boarding through choppy waters
🚨 TL;DR: The “Paddle Boarder’s Guide to Surviving the Medical System”
- The Problem: For neurodivergent and chronically ill people, a change in medical plans (like a surgery delay) isn’t just an “inconvenience.” It is an enormous, destabilizing wave that threatens to knock us completely into the water.
- The Metaphor: Most people navigate medical uncertainty on a stable cruise ship. They feel the waves but stay dry. We are on a stand-up paddle board. We require constant, exhaustive internal effort to balance on perfectly calm water. When the system changes, a “ripple” to the cruise ship becomes a catastrophic “tsunami” for us.
- The Fatigue: We are exhausted not because we are “weak,” but because we are spending all our energy on a silent, Invisible Brace. Every admin call, sensory input, and physical pain is a wave hitting our wobbly board.
- The “Flip”: When we have a meltdown, shutdown, or cancel plans, the “board has flipped.” This isn’t a failure; it’s a necessary, protective reset. We need to “sink” for a minute to stop the adrenaline of trying not to fall.
- How to Help: Don’t tell us to “be flexible.” Help us stabilize. Be the solid object we can hold onto. Take over the phone calls and give us the grace to be “underwater” until the sea calms down.
How many of us have heard these words, “Be more flexible”? I didn’t realize that meant my surgery date would be doing yoga while I’m just trying to stay upright. Between the rogue waves of kidney stones and the sinking weight of low ferritin, my medical calendar has become a series of “maybe next weeks” for my lumbar fusion.
To most people, a schedule shift is an inconvenience—a slight tilt on the deck of a cruise ship. But for the neurodivergent and chronically ill, stability isn’t a given; it’s a manually operated system. We aren’t on the cruise ship. We are on a stand-up paddle board in the middle of a high-traffic wake. Each appointment that changes often means changing another appointment, changing a leave request, and navigating yet another unknown.
When the world tells us to “go with the flow,” they don’t see the Invisible Brace. They don’t see the constant, microscopic mental and physical adjustments we make just to keep our heads above the spray. In a medical system that moves like a speedboat, being “flexible” isn’t a personality trait—it’s an expensive, exhausting executive function tax that may eventually lead to our board flipping.
And sometimes, flipping the board is the only way to finally find some peace.
The First Wave
It started with a constant wave pushing my side. A kidney stone—the first rogue wave in a storm I didn’t see coming. Then came the low ferritin, the overwhelming fatigue, and the sudden, sickening realization that my carefully constructed medical plan was no longer a plan; it was a loose suggestion.
In the midst of this chaos, I kept receiving I felt like I just needed to be remain flexible.
But that is a lot to manage: Flexibility is a great trait for a gymnast, but it’s a terrifying requirement for a medical plan. Here is the reality of my recent experience:
The Paddle Board vs. The Cruise Ship
To understand why “going with the flow” is so utterly exhausting for neurodivergent and chronically ill people, you have to understand the difference in our vessels.
Most people experience medical delays or schedule shifts like they are on a massive cruise ship. The floor might tilt, the waves might get choppy, and it’s certainly annoying, but the hull is thick enough to absorb the impact. They stay dry. They stay standing.
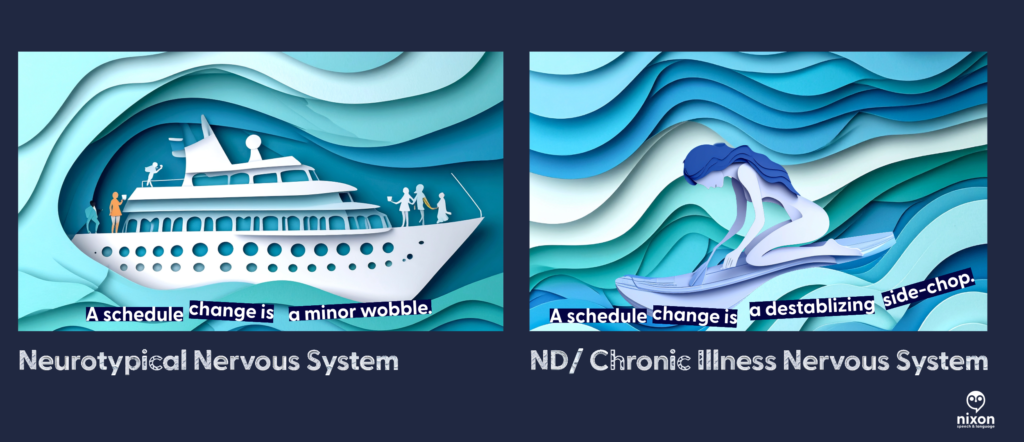
But when you are neurodivergent—craving predictability to manage sensory and cognitive loads—or living with chronic illness, you aren’t on a cruise ship. You are on a stand-up paddle board.
Even when the water is perfectly flat, we are already expending significant executive function and physical energy just to maintain balance. Every sensory input, every social interaction, and every administrative task requires a micro-adjustment of our internal stabilization systems.
When the medical boat (the scheduling office, the specialist, the test results) suddenly changes course, it creates a massive wake. For the cruise ship, it’s just more water. For the paddle boarder, it is a catastrophic side-chop that we were not braced for. Telling ourselves to “just stand up” when we have been knocked horizontal by the wake is a misunderstanding of physics.
The Invisible Brace: Taking on Water
If it’s not the main wake from the medical boat, it’s the debris. Being neurodivergent in a medical shift (or even change in what to do next) feels like you are paddling through a constant, exhausting stream of waves you cannot anticipate.
While we are trying to keep our balance, the environment is constantly throwing more waves at us, demanding more “flexibility”:
- The Rogue Wave (The Admin Avalanche): Having to make immediate phone calls to rearrange transportation, update employers, or coordinate with multiple specialists, all while processing bad news.
- The Side-Chop (Sensory & Cognitive Overload): Navigating an insurance company’s phone menu or reading complex medical instructions while in physical pain and brain fog.
- The Undertow (Sensory Dread): Mentally bracing for the specific sensory inputs of an impending procedure, only to have that dread extended indefinitely when the date moves.
This is Tether Fatigue. We are exhausted not because we are “difficult,” but because we have been in a permanent, tense, Invisible Brace for weeks, absorbing the kinetic energy of every ripple. Our energy reserves are fully bankrupted by the sheer volume of waves we’ve had to process just to avoid falling in.

The Grace of the Capsized Board
There comes a point where the balance is lost. The board flips. The paddle boarder goes under. To an observer, this looks like a crisis, a meltdown, or “giving up.”
But here is the secret that the neurotypical world needs to understand: Sometimes, we need to let the board flip.
When we hit the water, the Invisible Brace is finally over. We stop fighting the waves. We stop trying to anticipate the next administrative side-chop. For a moment, there is just the quiet, cold weight of the water.
We aren’t failing to cope; we are allowing the system to reboot because the cost of staying upright on a wobbly board hit by a tsunami has fully bankrupted our energy reserves. We need that “sink time” to stop the adrenaline and let our nervous systems reset before we can even think about climbing back onto the board.

How to Be an Anchor

If someone you love is neurodivergent or chronically ill and their “ship” has just flipped, don’t stand on the shore and yell at them to swim harder. Help them stabilize the water.
- Reduce the “Administrative Friction”: When the plan changes, the “to-do” list explodes, requiring executive function we don’t have.
- Don’t say: “Let me know if you need anything.”
- Do say: “I am standing by a phone. Give me your permission, and I will handle the rescheduling calls today so you don’t have to explain your situation five more times.”
- Validate the Physics, Not the Feeling: Don’t gaslight us with positivity. Acknowledge the environment.
- Don’t say: “Just keep rowing! Be resilient!”
- Do say: “The water is incredibly choppy right now. It makes total sense that you fell. I’m right here when you’re ready to try again.”
- Grant the Grace to Sink: Let us stay underwater for a minute. We need that silence to recalibrate before we have the strength to climb back onto the wobbly board.
Examples of Stabilization in Action
Example A: Dear Medical Provider (The View from the Paddle Board)
“When you tell me a surgery is delayed or a result requires a pivot, you might see it as a minor scheduling shift. For my neurodivergent brain and my chronically ill body, it is a tsunami hitting a stationary paddle board. Please help me stay above water:
- Reduce the Administrative Friction: Don’t make me the middleman between specialists. Coordinate the update with my other providers so I don’t have to spend my limited energy repeating my trauma five times.
- Give Me a Fixed Point: Tell me exactly what the next step is. Ambiguity is a wave I cannot balance on.
Example B: Dear Friend (When My Board Flips)
“Right now, the floor is shaking. I am exhausted from trying to ‘stay upright’ on a board that feels every single ripple. When you see me overwhelmed, please know that I’m not being difficult—I’m bankrupt from navigating a constant stream of administrative and sensory cross-currents. Here is how to be my anchor:
- Don’t Ask, Just Do: Telling me ‘I’m bringing over safe food at 6:00 PM’ is infinitely more helpful than ‘Let me know what you need.’
- Let Me Sink: If I cancel, don’t take it personally. My board has flipped, and I promise I’ll climb back on when the sea calms down.”
Flexibility isn’t a personality trait; it’s an expensive resource. For the neurodivergent and chronically ill, “going with the flow” often means fighting the current just to avoid drowning. Sometimes, the best way to help us is to just let us float until the sea is still again.
Note about the art:
To capture the “layered” nature of neurodivergent life, I used a collaborative AI process to create the visuals for this post. I worked with Adobe Firefly to generate the base “paper-cut” style and used Gemini as an “Art Director” to refine the metaphors—ensuring the “administrative debris” and the “underwater reset” felt as visceral as the words themselves.
Read more: BlogDon’t Lose Track of Health Insurance Calls: A free tool for patients and families

Have you ever spent hours on a call with a provider or insurance company and then when you call back you’re told they have no record of the call? If so, you know how exhausting self-advocacy can be.
Managing healthcare for yourself or your family shouldn’t require a law degree, but keeping a detailed “paper trail” is one of the most important things you can do when disputing a bill, fighting for a prior authorization, or coordinating care.
As a patient and provider, I know that advocating for care and coverage is hard enough. So I am sharing a tool I made for me and my husband in January 2026: A Healthcare and Insurance Communication Log. (See my last post for more information.)
This tool was made primarily for dealing with health insurance (including our pharmacy benefit manager).
What is it?
A simple, customizable Google Form that you can fill out on your phone or computer during or immediately after a phone call. Use it to track:
- Date and time of the conversation
- Who you spoke to
- What you discussed
- What your next steps (and their next steps) are
- And more…
You can quickly reference the key information needed from previous calls by looking at the entries in the form: (e.g., name of who you spoke with, company they are with, and date/time of the last communication, what was said, etc.).

A Quick Word on Privacy: Share the Tool, Not Your Data
If you find this call log helpful, we absolutely want you to share it with your friends, neighbors, or online support groups! However, it is crucial that you share the tool safely.
Because your copied Google Form is tied directly to your personal Google account and your private spreadsheet, sharing your specific form link outside of your immediate family (more specifically those involved in your healthcare and health insurance decisions).
If you send someone your personal link to copy for their own use, you will accidentally give them access to your Protected Health Information (PHI) and private medical notes.
The safe way to share:
The safe way to share: If you want to recommend this tool to someone else, do not share your Google Form link. Instead, simply copy the web address (URL) of this blog post and send that to them! This ensures they can read the instructions and download their own clean, private template that is completely separate from your data.
Disclaimer:
The Short Version: (Simply put)
- This is just a helpful tool: This tracker is a free organizational aid, not official medical or legal advice, and downloading it does not make you a patient of Nixon Speech and Language.
- This tool does not set reminders for you.
- You are in charge of your data: The information you type goes straight into your personal Google account, not ours. You are responsible for keeping your own account and passwords secure.
- Be mindful of privacy: Free Google accounts are not strictly protected by HIPAA (healthcare privacy laws). Please be careful about typing highly sensitive information (like Social Security numbers) into the form, and make sure you track strict insurance deadlines on your main calendar, too.
- Share the tool, not your data. Share the link to the blog to help your friends, not your own form.
Longer version
Please read before downloading: This form is a self-help organizational tool provided courtesy of Nixon Speech and Language, LLC. It is not a medical device, a legal record, and does not constitute professional medical or legal advice, nor does it establish a provider-patient relationship. Do not rely solely on this form for critical deadlines. By downloading this template, you acknowledge that you are the sole owner of the data entered and assume all responsibility for securing your personal Google account. Standard, free Google accounts are generally not HIPAA-compliant environments, so please exercise caution when entering highly sensitive Protected Health Information (PHI).
By downloading this template, you acknowledge that you are the sole owner of the data entered and assume all responsibility for securing your personal Google account. Standard, free Google accounts are generally not HIPAA-compliant environments, so please exercise caution when entering highly sensitive Protected Health Information (PHI).
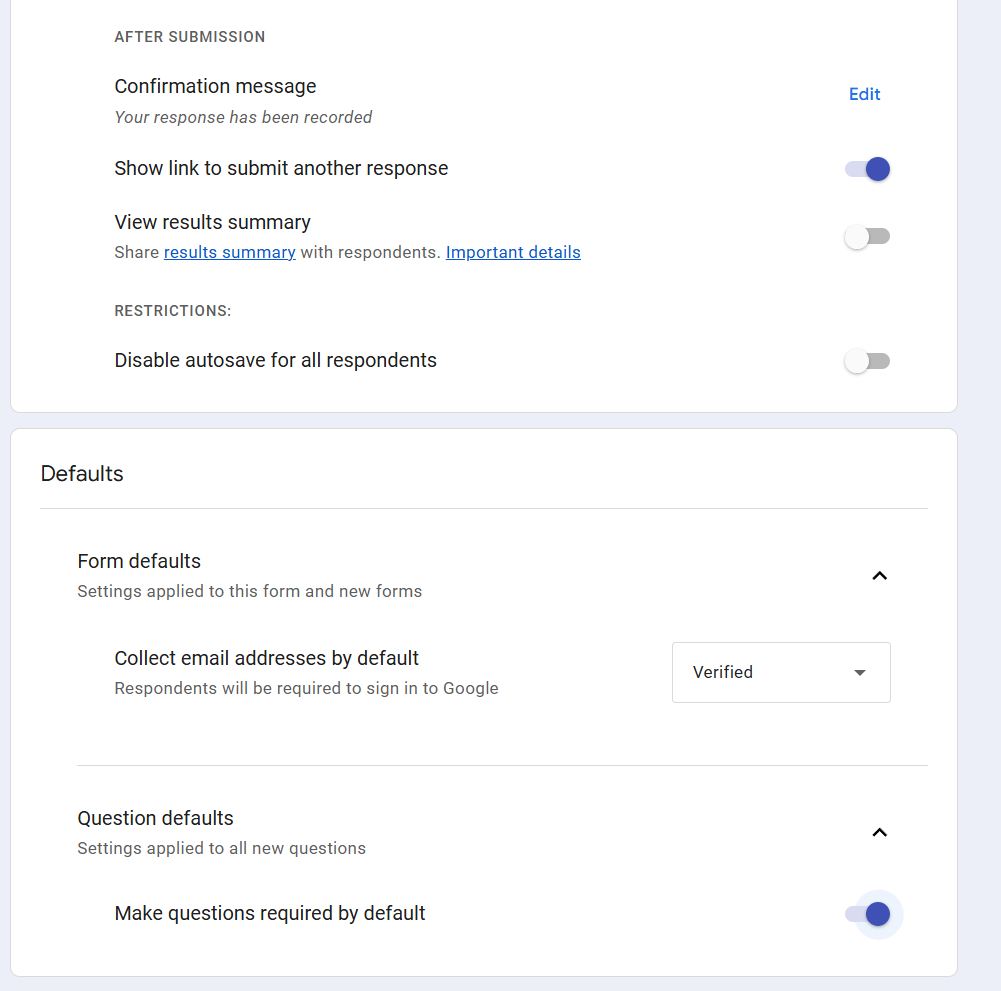
How to set it up
- Make your copy: Click the link at the bottom of this post and select “Make a copy.”
- Customize your form: Open your new form and edit the placeholder text.
- Change the “Who was the call about?” question to list your specific family members.
- Update the “Which organization did you contact?” question to list your main contacts (e.g., Blue Cross, Aetna, CVS Caremark).
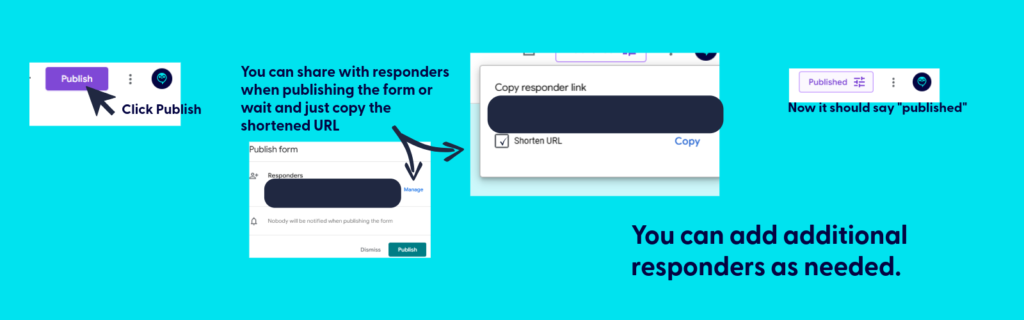
- Publish the form. Be sure to copy the link after publishing for your use.
- Save it for easy access:
- Fillable form: Bookmark the link to your fillable form on your computer (in Google Drive), or save it to your phone’s home screen so you can have it ready to complete during your next call.
- Bookmark the file used to create the fillable form: This is where you’ll find all your call logs. You can print (or PDF) specific responses or export all responses to sheets.
- Be sure to hit submit when you finish the call. If you don’t, your call log won’t save.

💡 Pro-Tip: Make it a Household Effort!
If you share healthcare duties with a spouse, partner, or adult child, you can use this single form to track everyone’s calls in one central place!
Once you have copied the form to your Google Drive and customized your family’s names, simply click the purple “Send” button at the top right of the screen. You can email the link directly to your partner, or copy the link and text it to them.
Have them save that link to their phone’s home screen. Now, whether it’s you calling the PBM about a prescription or your spouse calling the provider about a bill, all of your notes will feed into the exact same spreadsheet. No more asking, “Wait, what did the insurance rep tell you yesterday?”
The following applies only to those you want to share access to protected health information: If they need to be able to reference all calls for your household/family, be sure to share the backstage link AND fillable form.
📱 Make It an “App” on Your Phone
The easiest way to use this log is to save it directly to your phone’s home screen. That way, you don’t have to dig through your Google Drive every time you make a call.
First, get your fillable link: Open your form on your computer, click the purple “Send” button at the top right, click the link icon (the little chain), and copy that link. Email or text that link to your phone, then follow these steps:
For iPhone (Safari):
- Open the link on your phone using the Safari browser.
- Tap the Share icon at the very bottom of the screen (it looks like a square with an arrow pointing up).
- Scroll down the menu and tap Add to Home Screen.
- Type a short name for it (like “Insurance Log”) and tap Add in the top right corner.
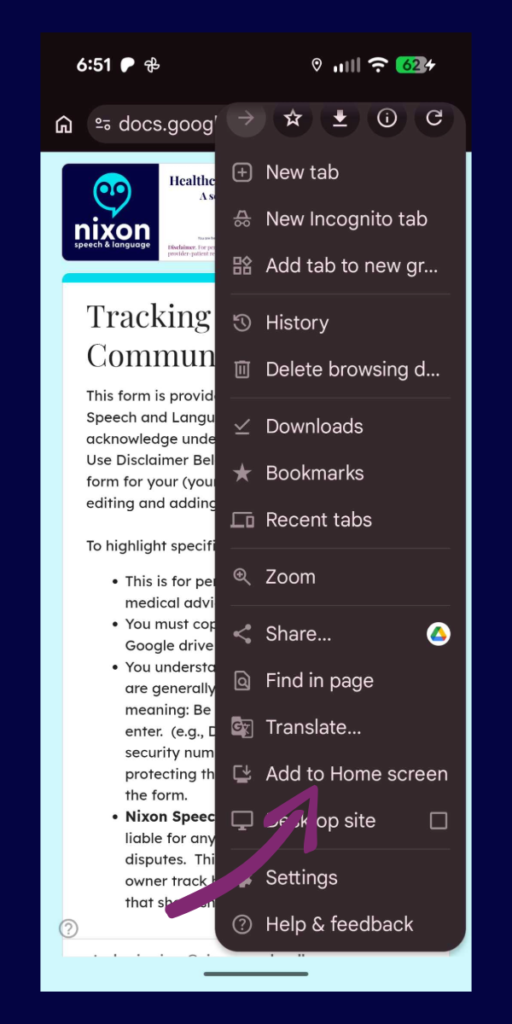
For Android (Chrome):
- Open the link on your phone using the Google Chrome browser.
- Tap the Menu icon in the top right corner (the three vertical dots).
- Scroll down and tap Add to Home screen.
- Type a short name for it (like “Insurance Log”) and tap Add.
Now you will have a shiny new icon on your phone right next to your other apps. Just tap it whenever you are on a call!
📂 How to View Your Call History (The form and spreadsheet)
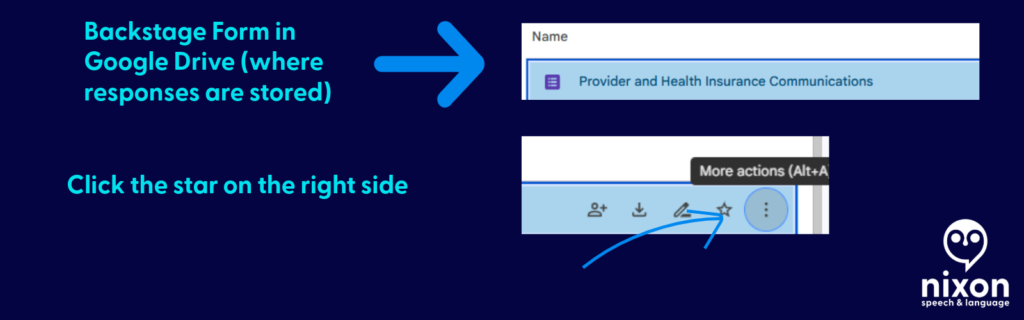
Think of your Google Form like a restaurant. The shortcut you saved to your phone is the “Front Door”—it’s just the menu where you place your new order. To see the history of every call you have ever logged, you have to go “Backstage” into your Google Drive.
Here is how to find your notes:
- Go to your Google Drive: On a computer, go to drive.google.com and log in with the exact same Google account you used to copy the template.
- Open the “Backstage” File: Find your saved form (e.g., “Healthcare Communication Log”) and double-click to open it. This opens the Editor view.
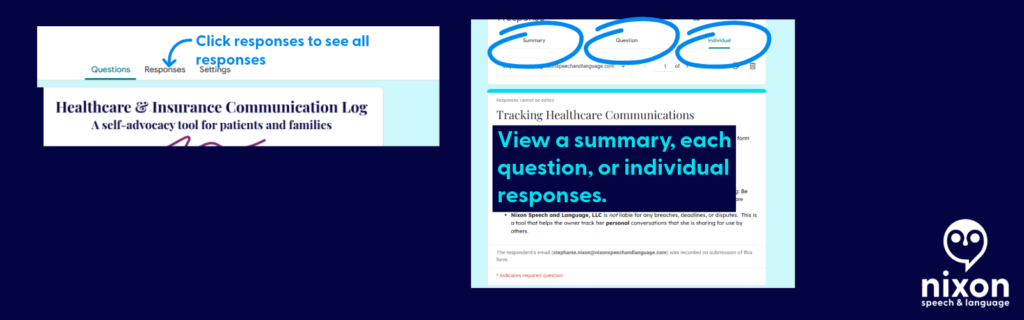
- Click the Responses Tab: At the very top center of the screen, click the word Responses (it is right next to “Questions”).
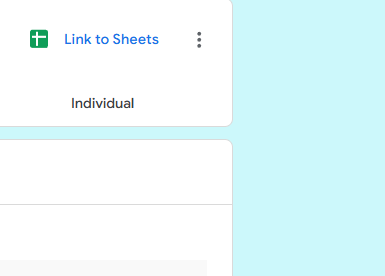
- Create Your Master Spreadsheet: For the best view, look for the little green icon that says “Link to Sheets” (or “View in Sheets”) near the top right of the Responses section.
Clicking that green button will instantly generate a clean, organized Google Spreadsheet containing every single detail of every call you have ever submitted.
📄 Need Hard Proof? How to Save a Call as a PDF
If you are filing a formal appeal or need to prove exactly how many times you contacted your insurance company about a specific issue, you can export individual call logs as clean, printable PDF documents.
Here is how to do it:
- Go “Backstage” into your form and click the Responses tab.
- Instead of looking at the spreadsheet, click the Individual tab (located right next to “Summary” and “Question”).
- You will see your form filled out exactly as you submitted it. Use the
<and>arrows to flip through your history until you find the specific call you need. - Click the Printer icon at the top right corner of that specific response.
- When your computer’s print menu pops up, change the “Destination” or “Printer” from your physical home printer to Save as PDF.
Now you have a professional, timestamped document you can attach directly to an appeal letter or an email to your provider!

Get the template
Ready to get organized? Click below to copy the template to your Google Drive:
Please read before downloading: This form is a self-help organizational tool provided courtesy of Nixon Speech and Language, LLC. It is not a medical device, a legal record, and does not constitute professional medical or legal advice, nor does it establish a provider-patient relationship. Do not rely solely on this form for critical deadlines. By downloading this template, you acknowledge that you are the sole owner of the data entered and assume all responsibility for securing your personal Google account. Standard, free Google accounts are generally not HIPAA-compliant environments, so please exercise caution when entering highly sensitive Protected Health Information (PHI).
By downloading this template, you acknowledge that you are the sole owner of the data entered and assume all responsibility for securing your personal Google account. Standard, free Google accounts are generally not HIPAA-compliant environments, so please exercise caution when entering highly sensitive Protected Health Information (PHI).
Remember, share the post, not your data.
By clicking here you acknowledge that you have reviewed the disclaimer.
Information provided in this post by, Stephanie M. Nixon, Ph.D., CCC-SLP, is provided in good faith. Nixon Speech and Language, LLC makes no representation or warranty of any kind, express or implied regarding the accuracy, adequacy, validity, reliability, availability, or completeness of any information.
“Patient’s Log”: Track your Insurance Calls Like a Provider (In 60 seconds)
Stop scribbling on scrap paper. Here is the exact system I use to hold insurance companies accountable (and keep track of what has been said).
In my last post, I talked about the importance of documenting every single interaction with your insurance company. But let’s be honest: when you are managing a chronic illness, working, or just living life, finding a notebook and a working pen while on hold is just one more hurdle.
My husband and I realized early on that we needed a system that was fast, shared, and impossible to lose.
Our solution? A simple Google Form.
It lives as an icon on our phone home screens. When we get on a call, we tap it, fill in the blanks while we talk, and hit submit. It automatically saves everything into a spreadsheet that we can search later.
Why This Works Better Than a Notebook
- It Prompts You: You never forget to ask “Who am I speaking with?” because the form requires you to type it in.
- It’s Collaborative: If my husband takes a call, I can see the notes instantly on my computer. No more “Did you call them?” arguments.
- It Creates a Timeline: When you need to file a grievance (like I did), you just open the spreadsheet and copy-paste the entire history.
The Fields You Need (Steal My Form)
I created a free Google Form with these specific questions. You can copy this exact structure:
- Patient calling about: (Checkbox: … Names of those in the household, etc.)
- Date called: (Date picker)
- Who contacted? (Checkboxes: Benefits, Care Management, CVS Caremark, HR, etc.)
- Method of contact: (Checkboxes: Phone, Email, Secure Message)
- Did I record the call? (Yes/No – Check your local laws as many areas require you to ask permission to record.)
- My Script: “I need to record this call so I have a record of what to do next. Do I have your permission to record?” Note. Be sure to note this to any new call participants.
- Note: If they say “No,” I immediately ask: “Since you are recording this for quality assurance, can I request a copy of that recording for my records?” (This usually changes the tone of the conversation!)
- Name of representative: (Crucial! Always ask for this first)
- Reason for call: (e.g., Prior Authorization, Billing Error, Benefits Question)
- Summary of call: (What did they say? What did you say?)
- How long were you on the call? (This is important evidence for complaints)
- Action items: (What did the representative promise to do? What do you need to do?)
- Follow-up date: (When should you check back?)

How to Set It Up
- Go to forms.google.com and click “Blank Form.”
- Add the questions listed above.
- Click “Send,” copy the link, and email it to yourself and your spouse/caregiver.
- Pro Tip: Open the link on your phone, tap “Share” (iOS) or the menu dots (Android), and select “Add to Home Screen.” Now it looks and acts just like an app.
The Result
When my pharmacy billing nightmare happened, I didn’t have to rely on my foggy memory. I opened my spreadsheet and saw exactly who disconnected on me on January 29th, and exactly what “Curtis” told me on February 6th.
That data wasn’t just notes; it was evidence. And evidence is the only thing that wins insurance appeals.
Disclaimer: I am a Speech-Language Pathologist and person with chronic illness, not an insurance broker or attorney. This post shares my personal experience and is not intended as legal or financial advice.
- When the board flips: Paddle boarding through choppy waters
- Don’t Lose Track of Health Insurance Calls: A free tool for patients and families
- “Patient’s Log”: Track your Insurance Calls Like a Provider (In 60 seconds)
- When $60 Becomes $800: How to Catch (and Fix) Health Insurance Errors
- Simple Kanban Task Tracker! Free!
When $60 Becomes $800: How to Catch (and Fix) Health Insurance Errors
A real-life lesson in why you must audit your Explanation of Benefits.
We often assume that when the pharmacist rings up a total, or when a medical bill arrives in the mail, the number is correct. We assume the insurance computer “knows” our plan.
But we also know that the insurance computer (and even the claims processors) have a history of applying the plan incorrectly (or inconsistently).
In January I had accepted that the “computer” knew our new plan for our prescriptions —and it nearly cost my family over $1,300 in a single month.

From Advocate to Patient
For years, I essentially worked two jobs. By day, I was a Speech-Language Pathologist working full-time. By night, I often spent three hours at a time, multiple nights a week, on the phone with insurance companies fighting for my own coverage. I learned early on that whether you are an educator advocating for a student, provider advocating for a patient, or a patient advocating for yourself, the system will often default to “No” unless you prove otherwise.
Now, living with chronic illness and on long-term disability, I no longer have that kind of energy to spare. My “work” today is largely just managing my own health. So when a computer glitch recently caused our pharmacy bills to skyrocket, it wasn’t just a financial error—it was a drain on the limited energy I have to survive.
I’m sharing this story not just as a professional who knows the paperwork, but as a patient who knows the exhaustion. I want to help you catch these errors quickly so you don’t have to spend your evenings fighting for the coverage you’ve already paid for.
The “Glitch”: When the Math Doesn’t Math
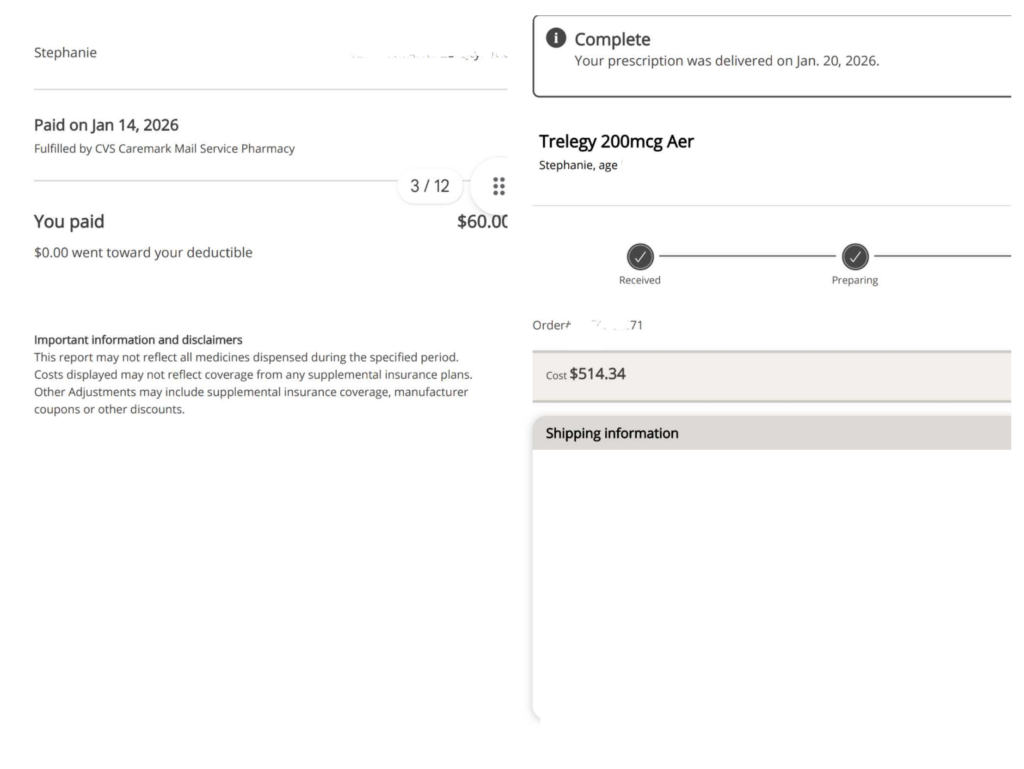
The “Glitch”: When the Math Doesn’t Math The situation started simply enough: My husband went to pick up a routine prescription. Instead of his usual $60 copay, he was charged $807.
The explanation from the pharmacy? “You haven’t met your deductible yet.”
That sounded plausible. It was January, the start of a new plan year. But when I logged into my portal, I saw something even stranger.
I had paid over $1,000 for medications in January, but my “Deductible Met” counter was sitting at $0.
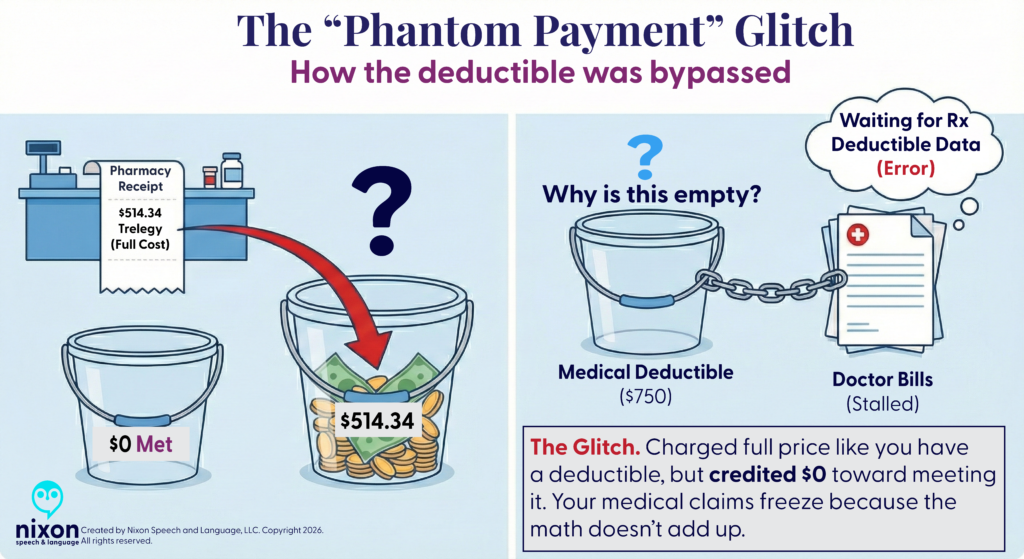
Where did the money go? The system had bypassed the deductible entirely and applied the cash directly to my “Max Out-of-Pocket” limit.
- The Error: They were charging me full price (as if I had a deductible), but refusing to credit my deductible bucket.
- The Result: I was on track to pay thousands of dollars out-of-pocket without ever technically “meeting” my deductible. It was a phantom charge that left me with the worst of both worlds: high costs and no progress toward my coverage limits.
The Domino Effect: Why You Can’t Just “Let It Slide”
You might be tempted to just pay the overcharge to avoid the hassle. I understand that urge completely. But here is the trap: Insurance systems use something called an “accumulator.” It tracks how much you’ve paid toward your deductible.
If you pay a deductible that you don’t actually owe, the system “learns” the wrong information. Later, when you see a doctor or go to the hospital, their claims might get stuck or rejected because the math doesn’t add up. By fixing this one pharmacy error, I wasn’t just saving money on a prescription—I was unblocking thousands of dollars in medical claims that were stalled in the system.
Red Flags: How to Spot an Error
Unfortunately, we had already paid for the medications. Although the error was corrected in the “Carefirst” and Caremark.com com systems as of February 2, 2026 (excepting my order receipts), we did not receive a refund or even notification that a refund was due.
In fact, after speaking with several representatives this week it seems the “correction” was backdated; however, neither Caremark nor the local pharmacy where we bough a medication were told we were owed refunds. Our local pharmacy credited us the money for their end, now I am trying to get a refund from Caremark.
Here is how to know if you should question a charge:
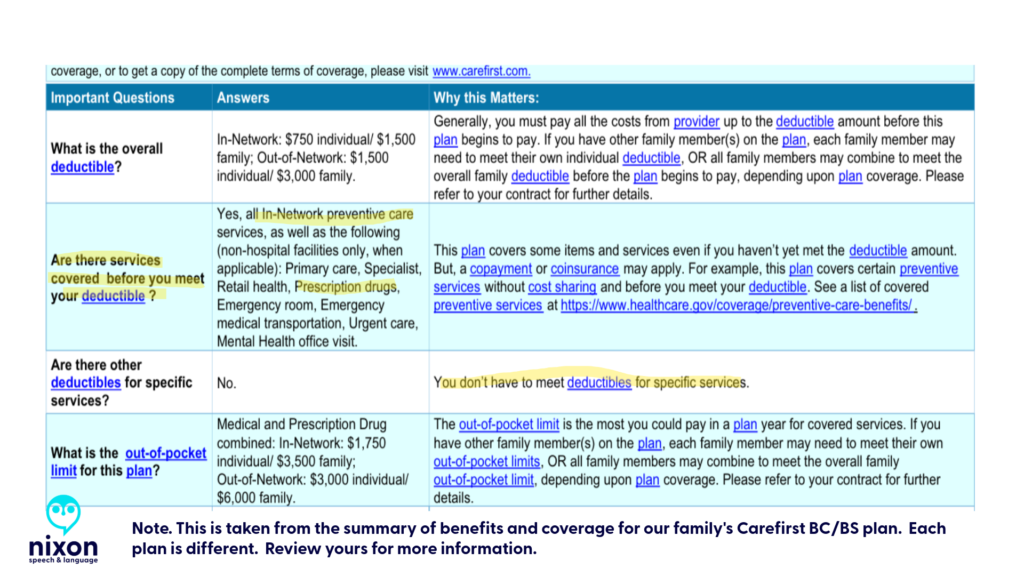
- The “Deductible” Surprise: If you have a PPO or HMO, your prescriptions usually have flat copays (e.g., $15, $30, $60) that apply immediately. If you see the word “Deductible” on a pharmacy receipt, check your plan design.
- The “Phantom Payment”: Check your insurance portal after a big purchase. If you paid $500 at the pharmacy, your “Deductible Remaining” should drop by $500. If the money disappears into the ether (or only hits your “Out-of-Pocket Max”), the system is miscoded.
- The “Processing” Limbo: If your medical claims (doctor visits) are sitting in “Processing” for weeks, it often means the medical system is waiting for the pharmacy system to send data that—thanks to this glitch—will never arrive.
Strategy: Write First, Call Second
The Reality: Phone calls are exhausting. But sometimes, secure messages result in frustrating, boilerplate responses that don’t answer your question. (I received a generic reply about “brand name drugs” that had nothing to do with my actual billing error!)
My advice: Even if you know you’ll have to call, send a Secure Message first.
- It creates a legal timestamp. Even if their reply is useless, you have proof that you reported the error on “Date X.” They can no longer say, “We have no record of that issue.”
- It forces a written response. When you finally do get a human on the phone, you can cut the small talk: “Please open Case #12345. I have already submitted the details in writing.”
- It respects your energy. If you have to file a formal legal grievance later, showing that they ignored your clear written explanation makes your case much stronger.
Pro-Tip: Document Like a Clinician
When you are dealing with brain fog or fatigue, relying on memory is risky. I treat every insurance interaction like a patient case note.
- Log Everything: Date, Time, and the Representative’s Name.
- Ask for the Reference Number: Every call has a “Case ID.” Ask for it immediately.
- The “30-Day” Clock: If they say they will “review it,” mark your calendar for exactly 30 days later. If they haven’t fixed it, they may owe you interest.
- See my post on creating a “patient’s log” that may help you track who said/did what (and when)
The Magic Words to Use
If you do have to speak to someone, use these terms to get past the front-line script:
- “Plan Design Error”: This tells them the computer is set up wrong for your specific group.
- “Adjudication Breakdown”: This asks for the math behind the price (e.g., how much was copay vs. deductible).
- “Accumulator Adjustment”: This asks them to fix your deductible history so future claims process correctly.
- “Senior team”: If you have already worked with the senior team on your issue, then explain the time it has taken and ask for the appropriate representative
The Takeaway
It took weeks of persistence, but we finally got a break. A representative worked with our local pharmacy on one claim and we were refunded for the discrepancy that was initially erroneously classified “deductible” ($747 of the $807.07 prescription cost). The call was disconnected before he could let me know how he was managing the issue with the Caremark pharmacy payments, but we have the proof we need to win.
I spent years advocating for others. Now, I’m learning that the most important advocacy is often the kind we do for ourselves—quietly, methodically, and with the receipts to prove it.
Disclaimer: I am a Speech-Language Pathologist and educational consultant, not an insurance broker or attorney. This post shares my personal experience and is not intended as legal or financial advice. Always consult your specific plan documents for coverage details.
Access and advocacy active listening andoid childhood apraxia of speech chronic illness claims processing communication log deductible Department of Education Discord doge Dyslexia dyslexia emoji dyslexia symbol education emoji errors processing claims google health insurance health insurance appeals health insurance benefits health insurance mistakes health unknowns Independent Funding innovation Institute of Education Sciences iOS18 iPhone Kanban Task Tracker learning disabilities managing your health max out of pocket National Institutes of Health neurodivergence NIH Organizer petition pharmacy benefit managers Planner pqbd.org research research design Research Funding speech-language pathology Systematic Research
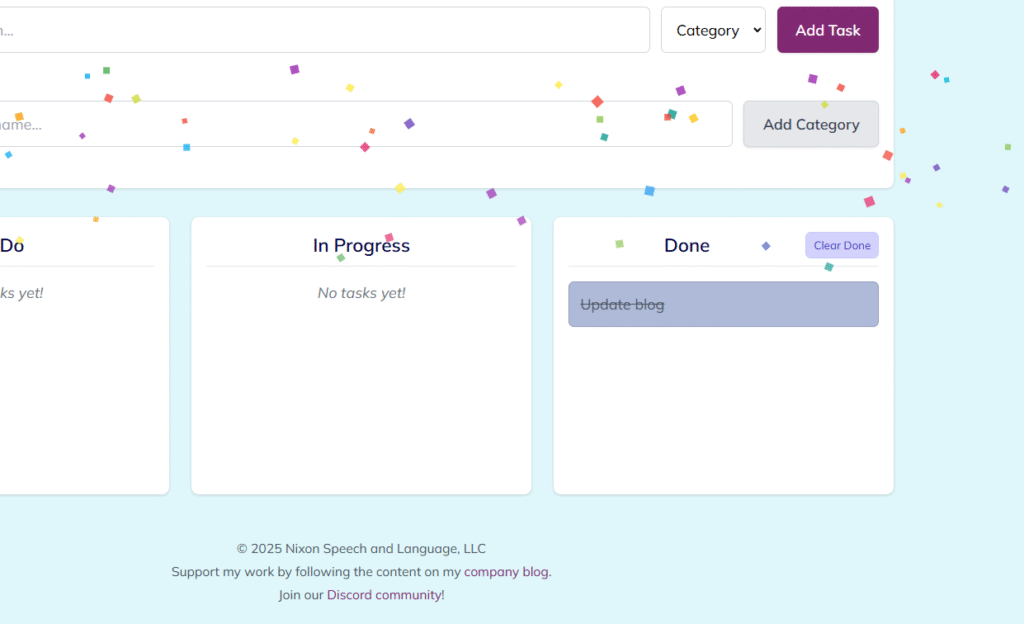
Simple Kanban Task Tracker! Free!
Organize your tasks visually with this easy-to-use Kanban board!
This tool helps you manage your workflow by moving tasks through “To Do”, “In Progress”, and “Done” columns. It runs directly in your web browser and saves your data locally, making it a simple, private way to stay organized.

Key Features:
- Visual Workflow: Classic Kanban layout with “To Do”, “In Progress”, and “Done” columns.
- Drag & Drop: Easily move tasks between columns using your mouse or touchscreen.

- Custom Categories: Add your own categories (e.g., “Project X”, “Follow Up”, “Home”) to better organize tasks. Predefined categories include “Work”, “Personal”, and “Urgent”.

- Color Coding: Tasks automatically change color based on their column (“To Do”, “In Progress”, “Done”) for quick visual status checks. Category badges also have distinct colors.
- Confetti Fun!: Get a burst of confetti whenever you move a task to the “Done” column. 🎉
- Local Storage: Your tasks and custom categories are saved directly in your browser, so they’ll be there when you reopen the app on the same device and browser.
- Clear Completed Tasks: Easily clear all tasks from the “Done” column with a dedicated button.
How to Download and Use:
- Download:
- Click the download link provided
- The license terms (GPLv3) are detailed below and available on the blog post/GNU website.
- Open: Double-click the downloaded
.htmlfile. It will open in your default web browser. No internet connection is needed after opening. - Add Tasks: Type a task description, select a category from the dropdown, and click “Add Task” or press Enter.

- Add Categories: Type a new category name in the “Add New Category” section and click “Add Category”. It will now appear in the dropdown list for tasks.
- Move Tasks: Click and drag (or tap and drag) tasks between the columns.
- Clear Done: Click the “Clear Done” button in the header of the “Done” column to remove all completed tasks.
Important Notes:
- Local Data Storage: Task and category data is saved only in the browser you are currently using on this specific device. It will not sync automatically across different computers, tablets, phones, or even different web browsers (like Chrome vs. Firefox) on the same device.
- Updates: For the latest version of this tool, please check the Nixon Speech and Language Blog or our Discord Community. Follow our blog or social media channels (linked below) for update announcements.
License:
This program is free software distributed under the terms of the GNU General Public License Version 3 (GPLv3). Essentially, this license guarantees you the freedom to use, study, share, and improve the software. You can redistribute it and/or modify it under the terms of this license.
Key points to understand:
- Freedom: You are free to use, modify, and share this software.
- Attribution: If you share or redistribute this software (modified or not), you must keep the original copyright notice (
© 2025 Nixon Speech and Language, LLC) intact. - Sharing Changes: If you modify the software and distribute your version, you must also license your modified version under the GPLv3 and make the source code available. You cannot make a modified version proprietary (closed-source).
- Commercial Use: You can charge a fee for distributing copies or offering support/warranty for the software, provided you follow all GPLv3 terms (like providing the source code and keeping it under the GPL).
- NO WARRANTY: This software is provided “AS IS” without any warranty. Nixon Speech and Language, LLC is not liable for any issues or damages arising from the use or modification of this software by others, as detailed in the full license text.
- Brand Protection: The GPL license applies to the code. The Nixon Speech and Language name and logo are trademarks and are not automatically licensed for use by the GPL.
The full terms can be viewed on the GNU GPL website. Please refer to the full text for complete details.
Developed with assistance from Google AI. © 2025 Nixon Speech and Language, LLC
Access and advocacy active listening andoid childhood apraxia of speech chronic illness claims processing communication log deductible Department of Education Discord doge Dyslexia dyslexia emoji dyslexia symbol education emoji errors processing claims google health insurance health insurance appeals health insurance benefits health insurance mistakes health unknowns Independent Funding innovation Institute of Education Sciences iOS18 iPhone Kanban Task Tracker learning disabilities managing your health max out of pocket National Institutes of Health neurodivergence NIH Organizer petition pharmacy benefit managers Planner pqbd.org research research design Research Funding speech-language pathology Systematic Research
GPL License
See the the GNU GPL website for additional information.
This license applies to the following hosted on our site:
- Nixon Speech and Language, LLC Kanban task tracker © 2025 Nixon Speech and Language, LLC
GNU GENERAL PUBLIC LICENSE
Version 3, 29 June 2007
Copyright (C) 2007 Free Software Foundation, Inc.
Progress
What is progress?
Merriam-Webster includes the following in the definitions of progress:
- “a forward or onward movement (as to an objective or to a goal) : ADVANCE”
- “a gradual betterment especially: the progressive development of human kind”
- “to move forward: PROCEED”
- “to develop a higher, better, or more advanced stage”

Image created by Dr. Nixon’s description provided to Adobe AI.
Imagine.
Pause. Imagine that it’s 1990. You are in a wheelchair. You do the same work as your peers, but you get paid less. You can’t go to a movie theater because there aren’t accessible seats.
Do we really want to go back to that?
That was life before the Americans with Disabilities Act of 1990 that includes Section 504. Section 504, the section being the one currently being challenged by attorneys general in 17 different states with Texas v. Becerra.
In an essay written in Time on February 19, 2025, Rebekah Taussig wrote:
“In many ways, Section 504 has operated as an almost invisible protection – easy to take for granted. And in doing so, we’ve been able to continue the fiction that disability is something that happens only to others. The undeniable fact is that every one of us will acquire a disability if we live long enough. Disability is an experience we can move in and out of over the course of our lives, and disabled people are the only minority group anyone can become a part of at any moment. Section 504 is not a law for “those people.” …
As with much of U.S. politics right now, Texas v Becerra feels like a reckless attempt to pull us back to a former time. But there is one crucial difference between 1977 and 2025. More than one generation of disabled children has grown up under the protections Section 504 provides us. And while the politicians are still reciting the same script, our revolutionary predecessors gave us a new story. We are a valuable part of our communities, we belong here, and we’ve been shown how to fight.”
Civil Rights Protections aren’t Red Tape
Why do you think civil rights laws such as ADA, the Civil Rights of 1964, and Individuals with Disability Education Act of 1990 (among others) were passed?
It was because people were (and still are, just check Supreme Court Cases) treated differently based on their race, religion, national origin, (dis)ability, gender (and gender identity), and sexual orientation.

Recently, the Trump administration froze the Civil Rights Division of the Department of Justice and changed the board of the EEOC in a manner that has many concerned. These groups are there to protect people’s civil rights against discrimination by employers, schools, businesses, landlords, law enforcement, and more.
If you think that shouldn’t be a concern, just take a look at what Rep. Rich McCormick (R-Ga) said when asked about school lunches after Trump proposed a federal funding freeze that could affect nutrition support for children: “Before I was even 13 years old, I was picking berries in the field, before child labor laws that precluded that. I was a paperboy and when was I was in high school; I worked my entire way through”.
Use of the phrase “back in my day” to dismiss concerns
Just because something was one way in 1954, doesn’t mean it should continue – particularly when it comes to civil rights.

Disclaimer. This post is not medical or legal advice.
The information provided in this blog post is for educational and informational purposes only. It is based on historical research, analysis, and interpretation, which may be subject to varying perspectives and ongoing scholarly debate. While every effort has been made to ensure the accuracy of the information presented, I do not guarantee its completeness or infallibility. Historical accounts can be complex and nuanced, and my interpretations reflect my understanding of the available sources at the time of writing.
This blog post may also contain personal opinions and reflections on the historical events and figures discussed. These opinions are my own and do not necessarily represent the views of others. They are offered as a basis for discussion and further exploration of the topic.
Readers are encouraged to conduct their own research and consult multiple sources to form their own informed opinions. I am open to respectful discussion and feedback on the content of this blog post, and I acknowledge that historical understanding can evolve over time. Any errors or omissions brought to my attention will be considered and, where appropriate, corrected.
By reading this blog post, you acknowledge that you understand and agree to the terms of this disclaimer.
Why should I care about cuts to federal research grants?

It isn’t just the “ivory tower”
Many people talk about university researchers as living in the “ivory tower” unaware of the needs of people in society.
I challenge you to pause for about 10 minutes and watch this video courtesy of PBS News to better understand potential long-term impacts of Trump’s cuts to research funding.
(And yes, I know the video is about medical research funding, but the same applies to education. Also, NIH funds more than medication research. They fund research into child development, reading, language, speech production, and so much more.)
Beyond that video, did you know that research grant funds also help pay tuition for students working in those labs? Yes. They can make higher education more affordable.
It’s part of the reason most grad and doctoral students look for labs with funding.
If research funding is decreased, then we may end up with less socioeconomic diversity in higher education due to the cost.
If research funding is decreased, then students who choose to pursue higher education degrees are likely to have higher student debt.
What can you do?
- Contact your representative and senator
- Speak UP! Post on social media!
Disclaimer. Information provided in this post by, Stephanie M. Nixon, Ph.D., CCC-SLP, is provided in good faith. Nixon Speech and Language, LLC makes no representation or warranty of any kind, express or implied regarding the accuracy, adequacy, validity, reliability, availability, or completeness of any information supplied by other sources.
Information provided here is for informational purposes only.
Call to action: Institute of Education Sciences: What is it? Why should I care?
Note. Should I omit information, please email or comment. As always, I will do my best to add relevant information here or in a future post.
Call to action: Please sign the petition
If you don’t need this article to realize the necessity of the Institute of Education Sciences (IES) and their role in funding high quality independent educational grant research, then please sign this petition in an effort to halt actions by DOGE and the current Presidential administration: https://chng.it/vjdYGZw9wz
If you just need the numbers to sign the petition:
- 2024 entire Federal Budget was $6.75 trillion.
- IES had an $807 million budget in 2024
- Between $800 million and $1 billion in IES research grants were cut by DOGE (Grants are paid over multiple years. See the note below.)
- Note. In this Washington Post Article posted 2/13/2025 by Meckler and Natanson, Nat Malkus, a senior fellow at American Enterprise Institute DOGE may have overstated the cost of the canceled contracts because many of the contractors were several years into the agreements, meaning the money has already been spent.
- In other words, canceling the grants right now likely caused more waste, especially if the studies cannot be completed due to lack of funding.
Other reasons to sign:
- IES is part of the accountability arm of the education system
- Studies are being cut short including one called, ReSolve designed to help students learn math faster.
- Federal funding cuts including grant funding to researchers at the institutions is devastating. This article in the GW Hatchet by Jenna Lee (2/11/2025) addresses lawsuits related to the NIH Federal funding cuts
- DOGE cut additional resources within that funding including:
- Common Core of Data, primary database of all K-12 schools with enrollment, demographics, and other information is collected
- What Works Clearinghouse: a project that has been essential to facilitating decisions for administrators and educators (see below for more)
- School Pulse Panel: began surveying K-12 public schools about education related topics
- Studies about international education
- Career and technical education
- Early childhood education
Contact your congressmembers. Protect this funding so our country can move forward with improving our education system on the whole vs. backwards. We need independently funded research. It is paramount.

If you need more convincing or just want some background, then read on.
Briefly…why do we have a Federal Department of Education?
Before we can discuss the Institute of Education Sciences (IES), we need to consider, why do we have a Federal Department of Education (DoEd)? Can’t the states do everything?
Time machine:
Let’s hop in our “time machines” and review history:
- 1867: The 39th US Congress passed the legislation to establish the first DoEd, which was signed by President Andrew Jackson. Some historical information is available via this article by Cross and Islas.
- Non-cabinet level agency with Henry Barnard as the first commissioner (and a staff of 3 and only 2 rooms)
- Objectives:
- improve American education by providing strong education information to local- and state-level authorities without having official control of the authorities in the states
- collect statistics and facts to show educational progress across states and territories
Henry Barnard
He deserves his own post (if I have time). For now, review the Barnard Papers and the information from Cross and Islas. Barnard had to collect data from the schools and send it to practitioners. He and his small staff produced reports and research to help give a context for education.
- July 20, 1868: Congress decided the the efforts by Barnard was a waste of national resources, reduced the funding, and then on June 30, 1869 removed the DoEd’s independent status and relabeled it the Office of Education with the Department of Interior.
- 1870: John Eaton served as the US Commissioner of Education until 1886 with only a $6000 yearly budget.
- 1889 to 1906: Commissioner William Torrey Harris continued the data collection and expanded it to include public and private elementary school enrollment.
This path continued, the name changed and shifted. In 1953, the Department of Health, Education, and Welfare. More funds were available due to political and social circumstances.
In 1963, President Lyndon B. Johnson emphasized the need for education to fight poverty leading to the Higher Education Act (1965) and Elementary and Secondary Education Act (1965).
Now, it’s 1979, President Jimmy Carter signed into law the Department of Education Act
This established the Federal Department of Education as a cabinet-level department.
What kind of funding did DoED receive in 2024?
Per USAfacts.org, DoED received 4% of all federal funding in 2024, totaling $268.35 billion.
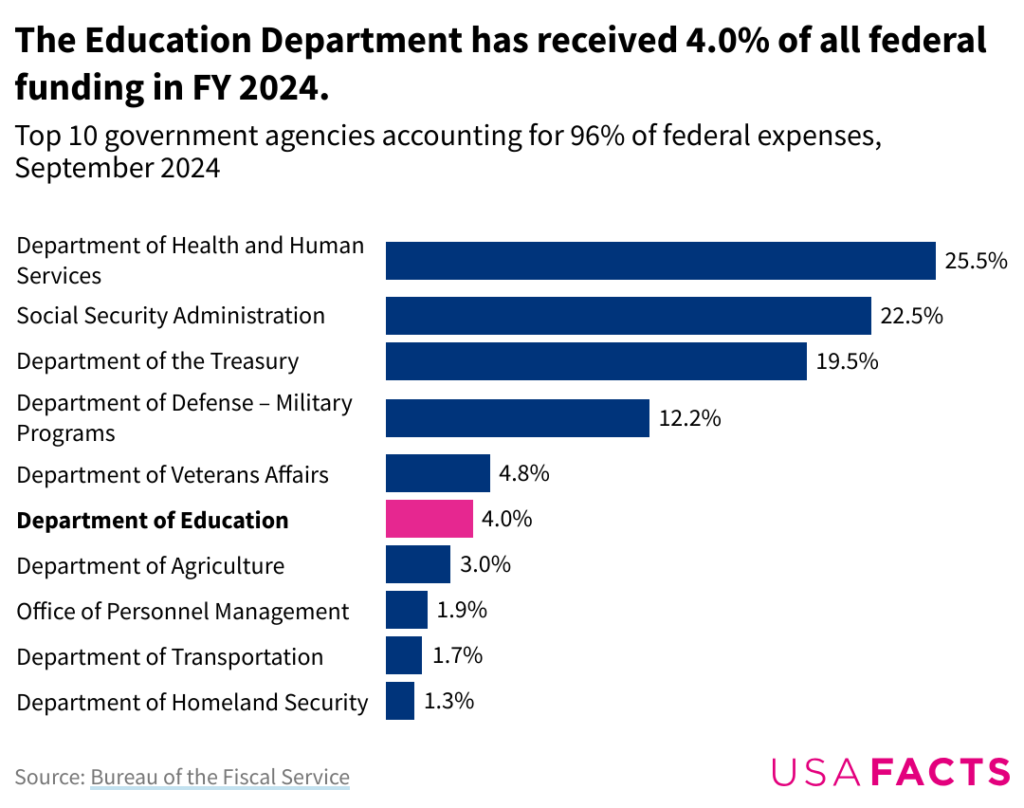
DoEd is the smallest of any cabinet-level department with about 4,100 full-time employees (as of 2023).
What is/was the function of DoEd as of 2024?
Note. Given the unknowns related to what data/websites will remain available under the current administration, I cannot guarantee the existence of any links to federal websites. If you click a link and it is gone, then please contact me and I will do what I can to find the information and make it accessible (when possible).
Under the Dept of Education Organization Act (PL 96-88), the DoEd was created to do the following: (The following is directly quoted from the linked page)
- “Strengthen the Federal commitment to assuring access to equal educational opportunity for every individual;
- Supplement and complement the efforts of states, the local school systems and other instrumentalities of the states, the private sector, public and private nonprofit educational research institutions, community-based organizations, parents, and students to improve the quality of education;
- Encourage the increased involvement of the public, parents, and students in Federal education programs;
- Promote improvements in the quality and usefulness of education through Federally supported research, evaluation, and sharing of information;
- Improve the coordination of Federal education programs;
- Improve the management of Federal education activities; and
- Increase the accountability of Federal education programs to the President, the Congress, and the public.”
As noted on the about page for DoEd, the mission “is to promote student achievement and preparation for global competitiveness by fostering educational excellence and ensuring equal access for students of all ages. Learn more about our mission, offices within ED, key initiatives, and more.”
What is the Institute of Education Sciences (IES)?
Brief Background
In 2002, President George W. Bush signed into law the Education Science Reform act (note, the link is to a compilation as amended and is unofficial) establishing the Institute of Education Sciences (IES).
“The mission of IES is to provide rigorous evidence on which to ground education practice and policy,” per https://www.ed.gov/about/ed-offices/ies.
Dr. Grover J. Whitehurst, the first director of IES, reviews the founding of IES in this journal article from 2018 entitled The Institute of Education Sciences: A Model for Federal Research Offices.
List of Some of the Products and Activities Conducted by IES
- National Assessment of Educational Progress: (Unknown)
- student achievement measure that is nationally representative and continuing assessment of what students know and can in several subjects
- data is used to help guide decisions to improve education in the country
- What Works Clearing House: (cut)
- collection of research-based evidence about programs and practices
- goal is to help stakeholders (educators, policymakers, and researchers) find the best practices for classrooms and schools
- National Center for Education Evaluation and Regional Assistance: (cut)
- provides unbiased, large-scale evaluations of education programs receiving federal funding
- provides training and coaching to states, districts and higher education institutions
- encourages development and use of research and evaluation in systems across the US
- National Center for Education Research: (Grant funding cut)
- promotes high quality and rigorous education science research
- funds research and training programs that can help improve practice, systems, and policy to optimize US education outcomes
- National Center for Special Education Research: (Grant funding cut)
- promotes high quality comprehensive research to expand knowledge of children and youth with or at risk for disabilities
- age range is infancy through post-secondary education
- ERIC: Repository of education related information including journal articles, dissertations, and other such resources
Importance of IES
IES is how we improve education. Under this institute, there have been education advances. Chester Finn wrote commentary on February 12, 2025 about this current situation with funding cuts to IES by DOGE. IES in its current form “corrected much of what was weak and wasteful in the previous arrangement —and the new agency got off to a strong start under the leadership of Grover (Russ) Whitehurst, who strove with considerable success to see that its work would be conducted as proper scientific research—controlled experiments, etc.—and data gathered and reported with objectivity and integrity”.
Within the notes, Mr. Finn linked to an interview with Dr. Whitehurst about Evidence-Based Education Science and the Challenge of Learning to Read.
Information for this post was pulled from these webpages (citations also linked within the post itself as appropriate):
Disclaimer: Including these links is not intended as Nixon Speech and Language, LLC’s or my an endorsement OR agreement with information created by the authors, companies, institutes, or websites. If you find factually inaccurate information in my post or a link, then please let me know and I will adjust.
- History of the department of education:
- https://education.stateuniversity.com/pages/2527/U-S-Department-Education.html
- https://en.wikipedia.org/wiki/United_States_Department_of_Education
- https://findingaids.library.nyu.edu/fales/mss_033/
- https://www.edweek.org/policy-politics/jimmy-carters-education-legacy-stretched-from-the-school-board-to-the-white-house/2024/12
- https://usafacts.org/explainers/what-does-the-us-government-do/agency/us-department-of-education/
- History of IES:
- Actions by DOGE and the Trump administration (2025) specific to IES:
- https://fordhaminstitute.org/national/commentary/easy-doge-ies-matters
- https://www.usatoday.com/story/news/education/2025/02/11/doge-musk-education-department-research/78411180007/
- https://www.washingtonpost.com/education/2025/02/13/doge-education-department-cuts/
- https://www.yahoo.com/news/education-department-pauses-research-contracts-020456976.html
- https://www.propublica.org/article/department-of-education-institute-education-science-contracts-doge
Disclosure. I am writing this as a supporter of strong education science and research. I am writing this as educators need rigorous peer-reviewed randomized studies to facilitate decisions. In my opinion, they also need access to quickly disseminated information as is available in What Works Clearinghouse. I am concerned at the likely negative outcomes for all children, but particularly those with learning disabilities or at risk for learning disabilities.
I worked at the Institute of Education Sciences from January 2004 through about March 2005 in the National Center for Education Research. I saw the amazing research. I watched the peer reviews.
Disclaimer. Information provided in this post by, Stephanie M. Nixon, Ph.D., CCC-SLP, is provided in good faith. Nixon Speech and Language, LLC makes no representation or warranty of any kind, express or implied regarding the accuracy, adequacy, validity, reliability, availability, or completeness of any information.
The opinions expressed in this post, are exactly that, opinions of Stephanie M. Nixon, Ph.D., CCC-SLP.
Evidence-Based Practices: Quick Overview
Note. This is an updated version of an article I wrote in 2021 for Apraxia Kids. The main reference was to childhood apraxia of speech research, but this applies to research across the sciences.
Some current (2025) actions by the executive branch make information of utmost importance. Some changes threaten sources of independent research funding.
What is evidence-based practice?
You may have heard speech-language pathologists (SLPs) saying “evidence-based practices” when describing a specific treatment approach. Such practices are based on scientific evidence and professional experience while considering your child’s specific needs.
Scientific evidence is used by SLPs, educators, and medical professionals (among others) to guide interventions and strategies could help a person based on their specific needs.
There is not one approach that works for all people, especially not for all children with childhood apraxia of speech (CAS). There are some approaches that have not been studied at all or have been studied with research methods that don’t allow for very strong conclusions.
What is scientific evidence?
Scientific evidence is empirical data that is collected and interpreted using the scientific method. This is evidence that serves to support or counter a scientific theory or hypothesis and is derived from controlled studies.
Is all scientific evidence high quality?
Simply put, no.

What are the levels of evidence?

Let’s summarize…
- The lowest form of evidence = opinions based on “experience”
- Best form of evidence = pulling multiple randomized controlled trials into guidelines or a meta-analysis
Anecdotes are not evidence especially when these anecdotes are offered by (or on websites of) people/companies with a commercial interest.

Applications are peer reviewed by field experts who determine whether the application meets the criteria among other standards.

Why does commercial interest matter in speech-language pathology or education?
What is a commercial interest? Earning money by selling a product OR saving money by not providing a service. (The latter is more relevant to health insurance – at least for now.)
Example: Dr. Blah at company XYZ creates and markets a program to teach math. If it is sold to school districts, then they will make money. Now if XYZ and Dr. Blah are the only ones who research the program they are more likely to determine this “works”.
What can decrease the quality of evidence?
Specific to CAS treatment research studies, look for study limitations (e.g., small sample size, inconsistent implementation of treatment approach, lack of a control group or condition, pre-treatment differences between groups, analysis performed by non-blinded outcome assessors, etc.).
Do we have much of the Level 1 standard research for Childhood Apraxia of Speech treatment?
No. We have a few meta-analysis studies and systematic reviews available.
Here are some systematic research reviews (most summaries by the American Speech Language Hearing Association in their Evidence Maps):
- Murray, McCabe, and Ballard (2014) concluded that of the research articles they analyzed, at least 3 treatments had sufficient evidence for Phase III clinical trials. Those treatments were Dynamic Temporal and Tactile Cueing (DTTC), Integrated Phonological Awareness, and Rapid Syllable Transition Treatment.
- Morgan, Murray, and Liégeois (2018) selected randomized-controlled trials and quasi-randomized-controlled trials including children aged 3-16 years grouped by treatment types.
- Ng, McCabe, et al. (2022) found an evidence base for the use of Rapid Syllable Transition Treatment (ReST).
- Springle, Breeden, et al. (2020) found limited higher dose and frequency of motor programming treatments appeared most effective for children with CAS.
SLPs can look at the “evidence” to determine which approaches are most likely to work. The evidence includes the research available and the patient’s unique needs.
What characterizes a strong treatment research study?
The gold standard for a therapy approach study is a randomized controlled trial and/or meta-analysis.
To evaluate a study, we look at the sample size, randomization, consistency of analysis, and fidelity.
- Sample size:
- How many participants/observations?
- Diversity in the population? (i.e., Gender? Race? Ethnicity? Primary language? Age – depending? Diagnoses? Socioeconomic status (SES)? Geographic location? Gender identify and expression? Disability status?)
Why do we care about diversity in the sample ?
Simply put: Inclusivity matters. The linked 2023 article by Alice McCarthy details the need for inclusive clinical trials.
Yes, we’re dealing with speech-language therapy trials vs. drug trials; but, that doesn’t change the need to ensure a representative population. This might advise a research of possible barriers to care as well as how to address the barriers.
I will address more about the need to ensure inclusivity in research and health disparities. For now, please review this article by Megan A. Morris (2022), Striving Toward Equity in Health Care for People with Communication Disabilities. You can also review disparities associated with health insurance on my blog.
- Randomization: There are many types of randomization as described in the article linked (Lim & In, 2019). Randomization helps researchers eliminate/minimize accidental bias (including selection bias).
- e.g., We want to ensure that patients weren’t chosen to receive the “treatment” group merely because they seemed to have more or less speech sound errors.
Bias in research
Bias in research is beyond the scope of this article. If you’d like to learn more, here is one journal article by Pannucci and Wilkins (2010).
- Consistency: This is often used interchangeably with reliability.
- Internal consistency indicates that several items measuring the same idea generate similar responses.
- External consistency is the degree to which results are consistent with prior research.
- Specific to consistency of analysis, we want to know how reliable were measures of patient performance. What was the level of agreement between/among therapists? How about a novel therapist?
- Fidelity:
- Were the control and treatment interventions provided as intended? For example, did the SLPs administering the interventions stay within the guidelines provided by the research study? Did they introduce any concepts not included in the study?
- Was the same modality of treatment used across patients in each condition? (in-person, telehealth, etc.)
Example.
(1) SLP working with a child in the “control” group includes some of the techniques from the “treatment” being tested and child shows progress in the “control” intervention.
Does this mean the “control” intervention works? No. It means the SLP did not follow the research protocol in the “control” intervention.
(2) SLP working with a child in the “treatment” group includes techniques beyond those described by the researchers as part of the treatment program (e.g., visual aids, cues, etc.) and the child shows progress with the “treatment” intervention.
Does this mean the “treatment” intervention works? No. It means the SLP did not follow the research protocol in the “treatment” intervention.
Other important factors
We also need to consider the presence of other factors that could explain improvement or regression (including whether these were controlled in the study). and whether these are controlled (e.g., if a child also received treatment elsewhere, or if a child started school, or had a medical procedure).
- Was the child receiving treatment beyond that supplied in the study?
- Did the child start school while in the study?
- Did the child experience any medical changes during the study? (e.g., new medication, surgical procedure, new diagnoses, accident, etc.)
Maturation (i.e., getting older) is another factor to consider when reviewing treatment studies. That is, did the treatment group improve beyond what would be expected based with aging.
What if one approach with research support isn’t working for my child?
Well, if you have that concern, ask the practitioner. Practitioners usually track progress so they know when they need to adjust intervention (i.e., when the approach is not effective for the patient or when the patient masters an objective, etc.).
As a clinician, I ask myself these questions when an approach doesn’t seem to be “working”?
- How long have we tried the approach?
- Am I implementing the approach correctly? (It helps to review the approach.)
- Is the child engaged (i.e., attending) with us during our sessions?
- How consistent is the child’s attendance?
- Have we provided appropriate family education (if included) with the approach? (This includes home practice)
Sometimes an approach just isn’t the best option for a child (and their family) and we need to adapt. This could include modifying the approach slightly to adapt or even changing approaches to one more suited for the child.
Regardless, an approach should have an evidence base, even if it was only demonstrated in a “single-subject design case study”. This allows SLPs to generate ideas/hypotheses (sophisticated educated guesses) about what might work for a given child.
Disclaimer. Information provided in this post by, Stephanie M. Nixon, Ph.D., CCC-SLP, is provided in good faith. Nixon Speech and Language, LLC makes no representation or warranty of any kind, express or implied regarding the accuracy, adequacy, validity, reliability, availability, or completeness of any information.
Information provided here is for informational purposes only.
This material is not substitute for professional medical advice or treatment. Always seek the advice of a qualified professional with any questions you may have regarding conditions and treatments/therapies. Do not delay seeking professional medical or educational advice/evaluation or delay seeking it because of something you read on this website.
See these websites for more information about evidence-based practices and research:
- Guyatt, et al. (2008). What is “quality of evidence” and why is it important to clinicians?
- The Comparative Study of Anecdotal vs. Scientific Evidence in 2024 via Science pod
- The What Works Clearinghouse was created by IES as a resource of educational evidence-based information
- Handout from Reading Rockets about evidence-based practices
- Burns, Rodrich, & Chung. (2012). The levels of evidence and their role in evidence-based medicine.
- A tutorial about evidence-based practices in health courtesy of University of Canberra Library
- Evidence-based practice toolkit courtesy of the Krueger Library