Words Have Weight: Stopping the ‘Deranged Twitter Feed’¹ in Your Chart
Part 2a
All blog disclaimers here
Personal Narrative & Data Integrity:
- Designated Record Set: This series represents a personal, professional audit of my own legally obtained medical history and “Designated Record Set”.
- Factual Basis: All clinical data points—including the 169.4-minute gastric emptying result —are pulled directly from my documented clinical records.
- Advocacy Intent: My goal is to highlight systemic disparities in medical documentation and foster better clinical communication.
- Non-Defamation: This audit is a critique of the content and quality of documentation and the patterns of clinical bias, rather than an attack on specific individuals or institutions.
A Note on Neurodivergent Baseline:
Contextual Accuracy: Observations regarding communication style, energy, or behavior (often labeled “manic” or “pressured” in my records) must be viewed through the lens of my documented, lifelong ADHD diagnosis.
A ‘u’ was added (AuDHD) as a late diagnosis a few years ago providing a key to understanding why so many providers saw ‘manic’ behavior where there was actually just a neurodivergent person managing a health emergency. We have to stop labeling what we don’t understand.
Have you ever read a medical note about yourself and thought: Who is this person? You are not alone. In a research study by Melanie Sloan and colleagues,¹ one patient described her medical record as:
“A deranged Twitter feed… creating a completely unrecognizable image of me as a patient and a person.”²
That quote hits hard. It describes what happens when a provider writes something subjective, negative, or dismissive in your chart. One note can change how the next provider sees you. And then the next. And then the next.
Patient safety experts call this The Domino Effect.³ This is how chart bias spreads.
What is Chart Bias?
Chart bias happens when a provider writes words that sound like a judgment of your personality rather than a description of your health. These subjective adjectives can quietly shape your care before a new doctor even walks into the room.⁴
Watch for “performance” words like:
- Dramatic,Anxious, or “Histrionic”
- Difficult
- “Saga”, Somatic/Somatization, or “Exaggerating”
- “Well-appearing” (especially when objective data says otherwise)
These words act as a path through your hospital record. They can lead the next doctor to subconsciously view your physical symptoms as a “performance,” questioning your credibility before you even speak.⁵
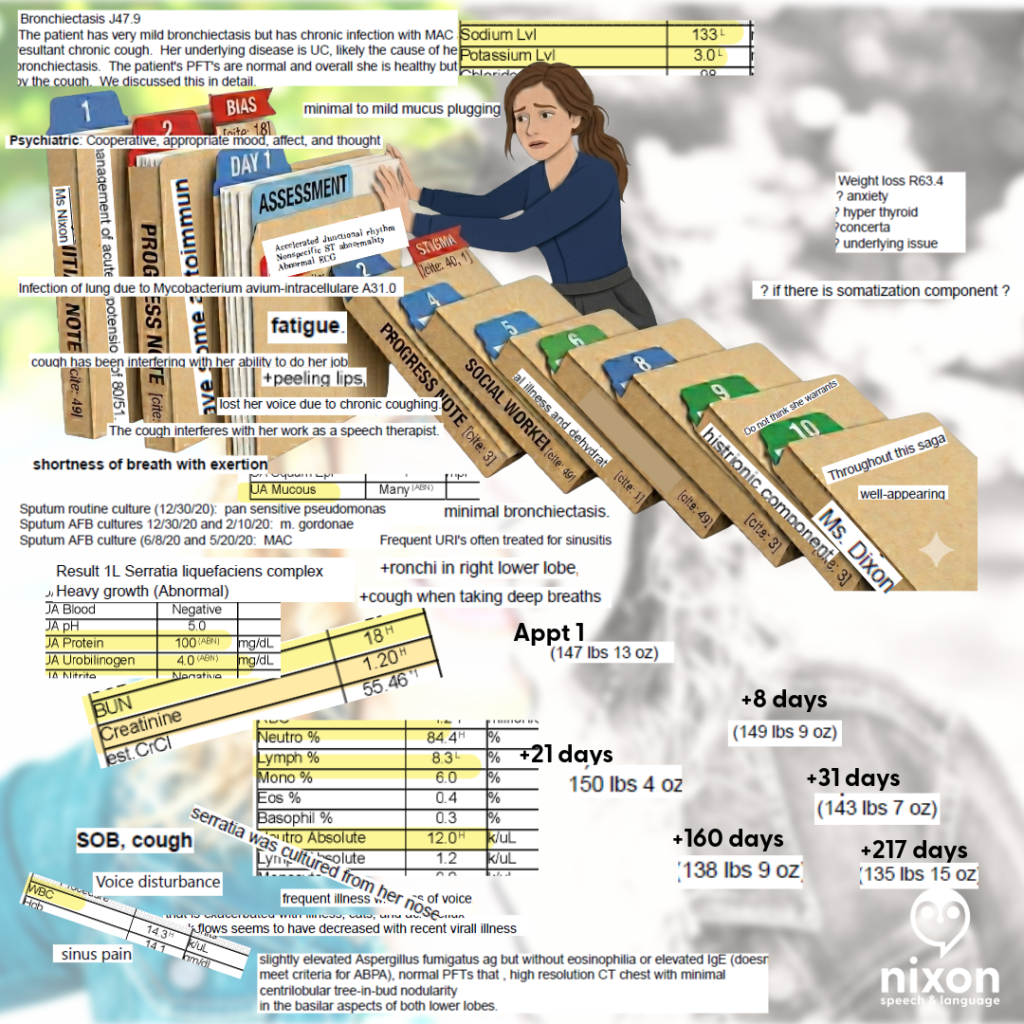
My Story: Same Patient, Different Stories
A few years ago, I saw my doctor for a cough that had lasted three months. I was hoarse and losing my voice. I provided a clear timeline and evidence of a bacterial infection. Instead of a diagnosis, the provider labeled my experience a “saga” and wrote that I was “demonstrating” my cough.The first note framed the encounter subjectively; the second documented objective evidence of infection.
I wasn’t “demonstrating”— when I didn’t cough, I was taking shallow breaths. Because one cough led to more coughing, and coughing led to bladder incontinence (even mild is embarrassing, iykyk).
Eight days later, a specialist looked at the same body but saw a different story:
- Abnormal lung sounds (Rhonchi)
- Rapid heart rate (Tachycardia)
- Chest CT results: “Tree-in-bud nodularity,” which showed a likely infection.
The first note framed the encounter subjectively; the second documented objective evidence of infection.
When the Story Overwrites the Facts
Later, in the ER, a doctor labeled my coughing “histrionic” despite contemporaneous objective findings including a blood pressure of 80/51 and an elevated white blood cell count paired with elevated neutrophils (84.4%) and low lymphocytes (8.3%). I will never know if the doctor was reading the “saga” in my chart, but somehow the data on the screen didn’t receive the same emphasis in that note as his perception of me as a “chronic pain” patient.
I eventually filed a HIPAA correction to have the word “histrionic” (and other comments) struck from my record. I did this because words in a chart don’t stay in one visit. They follow you.
To this day, I still question what I could’ve done differently to avoid being misunderstood. Yes, when I go to the ER, I try to communicate past my pain past my symptoms in hopes because in my mind that is the best way to get help. Sometimes, it works … Other times, it seems providers think if you can communicate that well you can’t be “that sick”.
Why This Matters
Research shows that even one stigmatizing note can change how clinicians think about you. It can change how seriously they take your pain and how hard they look for a physical cause.3, 4, 5, 6, 7 In other words: your chart can become a story about how the provider perceives your character instead of a record of your health.¹, ²
And when I realized what that provider said and what another provider said – providers I thought I trusted, it felt like betrayal – it hurt.
Those comments didn’t match with my personality or with what I was experiencing in those moments in those hours on those days. And the thought that a provider would put those words, words I would’ve told interns not to use ever, in my chart – the chart of another provider, felt like a slap.
Could I have just ignored these comments and found new providers? Yes. But they would stay there. So I have decided to advocate with whatever spoons I have.
The “Spoon Theory” of Medical Advocacy
Dealing with chronic infections, illness, providers, employers (concerned about productivity from missed work due to the first two-three), and trying to have a balanced life – well it is absolutely fatiguing.
That means many of us come into these situations with our executive function cups full to overflowing. Such situations require working memory – we need to hold in our memory what the provider says in the current appointment at System A, what the labs say, what our imaging says, what the other provider at System B, not to mention what we might need to take care of at work or home because we may need to schedule another appointment.
So when I saw the note above in my chart, the biased note, it was like a “gut punch” that felt invalidating. It drained my energy. And I know there are other patients (many women) out there like me. I thought the ER visit that night went okay – I thought the provider understood, then I saw that note.
Yes, can I look up all the terms to understand what each lab means? But the energy – it’s overwhelming:but that costs “spoons” you don’t have.
For me, I have been using an AI Buffer – to separate the data from the disrespect, the dismissal, the gut punch, literally not being heard…
What You Can Do? (Action Plan)
Safety note for readers.
For me, these are my strategies to navigate care today at this moment. I will provide more information about these paths later – but I hope these help:
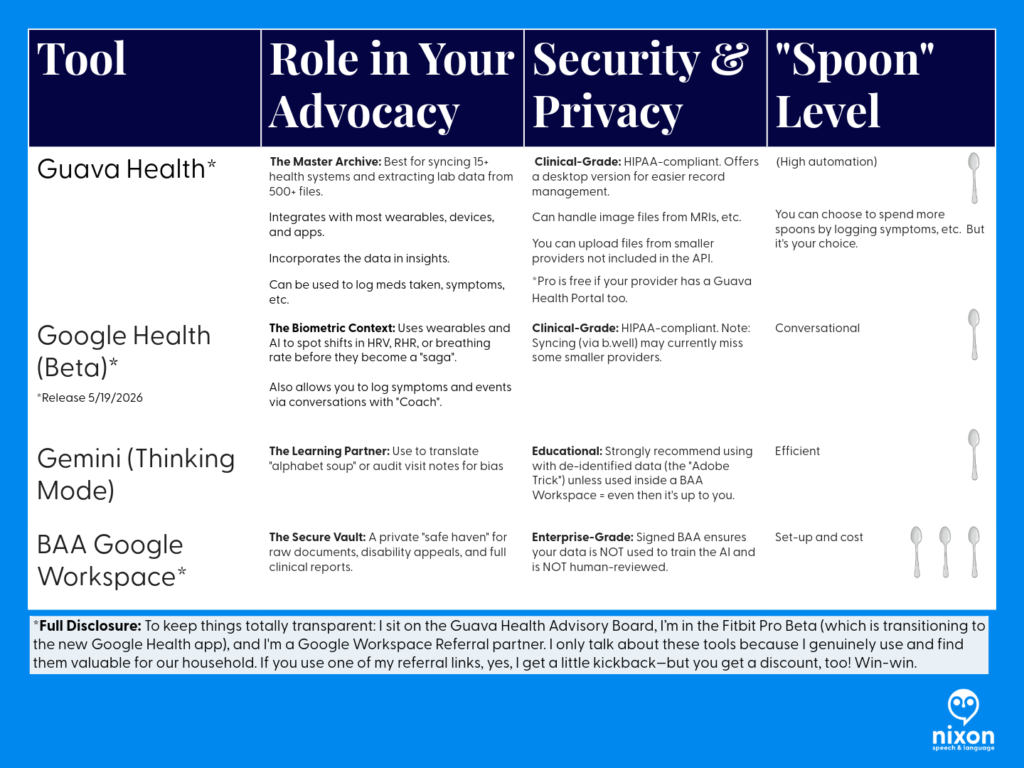
Strategy Summary
- Audit for Bias: Use Gemini (Thinking Mode) to help you objectively spot if a note describes your personality instead of your physiology.
- Externalize Your Memory: Use Guava’s Body Map and Medication Tracker to replace the high-stress “spotlight” of trying to remember 32 medications during a 15-minute visit.
- Provide the Receipts: Use your multi-year biometric trends (Heart Rate, HRV, etc.) to prove that your symptoms are a significant shift from your baseline, not “health anxiety”.
- Protect Your Privacy: If you are managing sensitive documents like disability appeals or vocational reports, move them into a Google Workspace with a BAA for maximum protection.
Why This Tech Matters
Using these tools isn’t about obsessing over every data point; it’s about Spoon Management. When you have a complex history—like Ulcerative Pancolitis or Gastrointestinal Dysmotility—you shouldn’t be expected to be your own medical librarian. These tools turn the “deranged Twitter feed” of a medical record into a searchable database that you control.
Here’s how how I go about it
1. Access Your Notes (Medical Records)
Under the Cures Act, you have the right to see your clinical notes.⁹ Don’t just read the summary; get the Progress Notes.
Tips: Sign up for the patient portal.
Use the summary like a snapshot. It’s the outline to the Progress Note (usually). But, often it just lists your current medications or the appointments to schedule, etc.
2. Create an “AI Buffer” (Protect Your Spoons)
Medical advocacy is exhausting. When a note feels like a “gut punch,” don’t waste your limited energy (“spoons”) manually looking up every term.
- The Strategy: Use an AI tool to objectively “audit” the note. Ask: “Does this note focus on my health or my personality?” (If it focuses on your personality – ask yourself if that is the provider’s role in your care.)
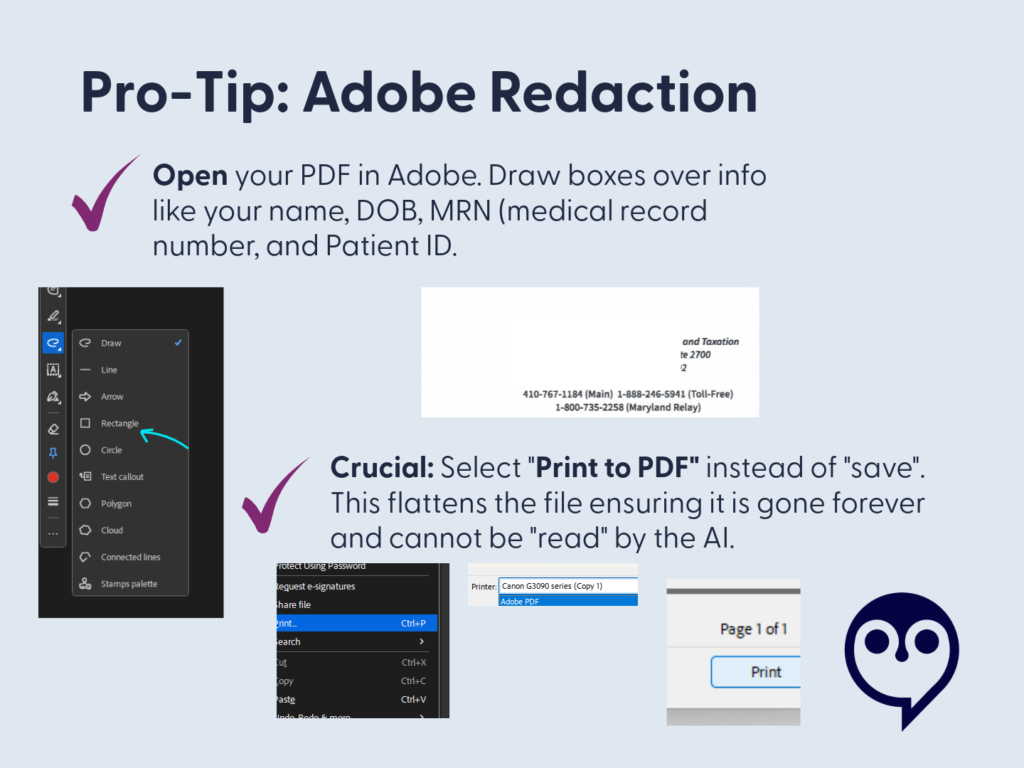
* The Privacy Choice: If you use an AI like Gemini, consider a Google Workspace with a BAA.11 This ensures your data isn’t used to train public models and isn’t reviewed by humans. It’s your “Safe Haven” for medical records. (I’ll talk more about this in another post – but I want to be sure you understand those risks.)
If you’re thinking about setting up Google Workspace for yourself, keep an eye out for my upcoming post on how I’m using it to manage our household! I’ll be sharing a deep dive, and as a member of the Google Workspace Referral Program, I’ll share some information and discount links – we will both be rewarded. <3
- Accuracy Tip: Always use “Thinking” or “Pro” mode for medical analysis. “Fast” modes can miss the technical nuances you need for an appeal.12
3. Use Technology to “Translate” and “Talk”
If you struggle with dense text due to dyslexia, a stroke, or a learning disability, use these apps to hear your data:
- Guava Guardian (Beta): A personal health detective. It can voice-alert you to a “split chart” (duplicate records) and helps you see how symptoms like hoarseness correlate with objective biometrics like HRV.
- Google Health Coach Pro (Coming May 19): This multimodal tool allows you to talk to your data. Instead of squinting at a screen, ask the Coach to “summarize my last labs in plain English.”
4. Request a Correction
If you see something inaccurate or stigmatizing, say something.There are several paths and each depends on your comfort level with the provider.
I’ve used emails, faxes, portal messages, and phone calls to navigate these issues. In the portal, be aware that other providers in that system can likely see your messages. (I didn’t know this.)
How to start:
- Contact the provider directly via the patient portal to request the correction/clarification: “I was reviewing my visit note from [Date] and noticed the history doesn’t match the objective data from my specialist. I’ve attached the relevant lab results and cultures to help clarify the timeline. Could we update the record to reflect these physical findings accurately?”
- Contact the hospital’s Medical Records or Patient Advocacy department and ask about the amendment process.
- For small practices, there is still a path for requesting corrections – this is your right to request it and there must be a path provided to you in that LONG HIPAA statement you received. Ask.
Phrases you can use:
- “I read my note and this wording does not reflect what happened.”
- “Can we focus the record on the objective lab findings from that visit?”
- “I would like to add an addendum to reflect the functional impact of my symptoms.”
I’ll go into this further in a separate post. I don’t want to tell you it will always work out. But I do want you to know this is your right. And I understand it isn’t as easy as I said just now.
The Bottom Line
Your medical chart should describe your health. It should not turn one provider’s opinion into your permanent identity. If you feel like your chart describes a stranger instead of you, you are not wrong to question it.
References
- Sloan, M., Naughton, F., Harwood, R., Lever, E., D’Cruz, D., Sutton, S., Walia, C., Howard, P., & Gordon, C. (2020). Is it me? The impact of patient-physician interactions on lupus patients’ psychological well-being, cognition and health-care-seeking behaviour. Rheumatology Advances in Practice, 4(2), rkaa037. https://doi.org/10.1093/rap/rkaa037
- Sloan, M., Bosley, M., Gordon, C., et al. (2025). “‘I still can’t forget those words’: mixed methods study of the persisting impact on patients reporting psychosomatic and psychiatric misdiagnoses.” Rheumatology. doi: 10.1093/rheumatology/keaf115. PMID: 40037287; PMCID: PMC12107051.
- Davis, B. (2021). “Derogatory Language in Charting: The Domino Effect.” Patient Safety Network. https://patientsafetyj.com/article/73542-derogatory-language-in-charting-the-domino-effect
- Goddu, A. P., O’Conor, K. J., Lanzkron, S., et al. (2018). “Do Words Matter? Stigmatizing Language and the Transmission of Bias in the Medical Record.” Journal of General Internal Medicine, 33(5), 685–691. doi: 10.1007/s11606-018-4583-7. PMID: 29374357; PMCID: PMC5910343.
- Park, J., Saha, S., Chee, B., Taylor, J., & Beach, M. C. (2021). “Physician Use of Stigmatizing Language in Patient Medical Records.” JAMA Network Open, 4(7), e2117052. doi:10.1001/jamanetworkopen.2021.17052
- Barcelona, V., Scharp, D., Idnay, B. R., et al. (2024). “Identifying stigmatizing language in clinical documentation: A scoping review of emerging literature.” PLOS ONE, 19(6). doi: 10.1371/journal.pone.0303653. PMID: 38941299; PMCID: PMC11213326
- Silverman, K. (2023). “Improving Health Equity by Eliminating Biased and Stigmatizing Language in Medical Notes.” Center for Health Care Strategies.
- CRICO (2021). “Cures Act Overview”. https://www.rmf.harvard.edu/Risk-Prevention-and-Education/Article-Catalog-Page/Articles/2021/Cures-Act-Overview
- Pandita, D., Johnson, D., & Bledsoe, T. A. “Lab Results Reporting, Ethics, and the 21st Century Cures Act Rule on Information Blocking.” ACP Ethics Case Study Series. https://www.acponline.org/clinical-information/medical-ethics-and-professionalism/ethics-case-studies-education-resources/lab-results-reporting-ethics-and-the-21st-century-cures-act-rule-on-information-blocking
- HHS.gov (2025). Your Medical Records. https://www.hhs.gov/hipaa/for-individuals/medical-records/index.html
- Google Workspace (2026). “Gemini for Workspace: Enterprise Privacy and Model Training Standards.” https://knowledge.workspace.google.com/admin/gemini/generative-ai-in-google-workspace-privacy-hub
Access and advocacy, Bias, chronic illness, clinical documentation bias, Clinician Associated Patient Trauma, empower patients, patient advocacy in healthcare, Words have Weight