Research vs. Reality: Why Perplexity Health Fails Chronic Patients Where Guava Health Thrives
Transparency Disclosure
In a world of sponsored “health tech” content, here is the truth:
- I am a paying subscriber of Perplexity Pro ($20/mo) and a paying subscriber of the Guava Health Family Plan.
- While I serve on the Guava Health Patient Advisory Panel, I do so pro bono (unpaid).
This review is not a promotion; it is a clinical audit. I’ve spent my own money on these tools because I am a “spoonie” patient, provider, and researcher searching for a way to make a complex life more manageable. (But for the record, I do accept cookies.)
The Dangerous Illusion of “All Your Data”
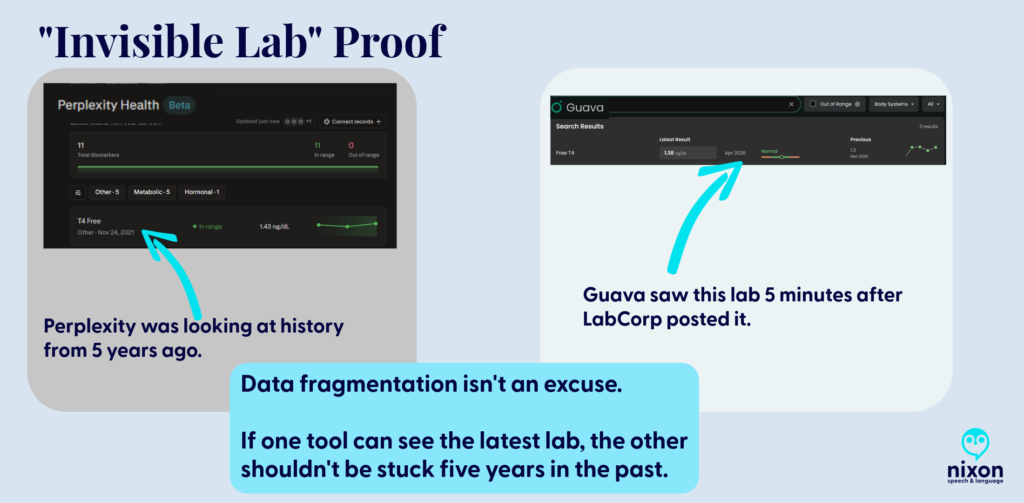
The biggest risk of Perplexity Health (Beta) is the illusion of completeness. Its marketing promises a seamless “Health Hub,” but my testing revealed a dangerous “blind spot.” Despite being connected to my EMRs, Perplexity ignored my most recent labs and defaulted to a T4 Free result from 2021 as my “current” status.
The Safety Warning: If a patient trusts Perplexity’s dashboard, they might miss key data and believe they are clinically stable when the AI is simply “ignoring” the last five years of their data because it didn’t index in a way the AI could add to your biomarkers.
The Guava Advantage: Guava understands that medical data is messy. Even when a provider doesn’t have a direct API integration, Guava allows you to upload the report. The platform doesn’t just “store” the PDF; it indexes and pulls that data into your biomarkers, ensuring your trends are accurate and complete (or as complete as the data it obtains via APIs and your uploads).
The “Spoonie Tax”: Friction as a Barrier
Chronic illness management is often a full-time job. We use technology to save “spoons,” not spend them. Perplexity, however, added to that fatigue through technical friction:
The Quantity and Size File Wall
I could only upload 200 documents. As a person with chronic illness who has been on this earth more than say 40 years, that didn’t begin to cover even half of my documents. You might tell me, ‘Just upload the most important ones’ or ‘Import them from the provider’, well, I tried that.
- The connection to my primary care provider’s office linked to her old facility vs. the current one despite having the correct address on file for her.
- My dermatologist, hematologist, integrative medicine provider, endocrinologist, cardiologist, gynecologist, primary care provider, and gastroenterologist weren’t accessible via Perplexity. (And these are only a few of the providers whose data couldn’t be accessed by Perplexity.)
- Note. Six of eight of the above aren’t accessible via Guava either, but I can upload those visit notes to Guava Health myself.
- To only see 10% of the data can also limit seeing the big picture. So, I grouped the files using Adobe to upload them (after deleting each individual file that I had uploaded).
- BUT if you’ve used AI to try to analyze data in large 150+ page files, you’ll know … it isn’t always easy. (Even Gemini tells me occasionally that my files are “too large”.)
The Administrative Demand
Then I had an interesting ‘conversation’ with Perplexity’s AI when I realized that despite syncing up with the API of one of my facilities with most of the lab data, it was missing specific data points (e.g., all Free T4 data after November 2021 despite that specific lab being drawn between 2-6 times/year.)
So I asked Perplexity Health’s AI where the labs are, and was told “You’re right that [FACILITY X] has them and that you uploaded them; the issue is that they’re not surfacing in the structured “labs/observations” stream I can see”. The AI provided several reasons for why those labs weren’t there:
- They may be stored only as a scanned PDF/image of the ER report, not as discrete lab rows, so they don’t appear in the lab feed even though they’re in your chart.
- The upload might be filed under “Media,” “Documents,” or an outside-records bucket that isn’t mapped into the lab/observation section my view is pulling from.
- The interface that shares data from Facility X’s EMR to this aggregate view may not map ED lab panels from that date or that specific visit type correctly.
But as a patient, provider, or researcher, the issue for those of us using Perplexity Health is that those labs aren’t there, and even uploading them, doesn’t lead to them being added to the biomarker section of the site.
So when I asked Perplexity AI what I should do, it suggested that I call the hospital’s IT department to request they “re-index” my FHIR API mapping.

Even when I provided the connections to the facilities and uploaded the records (labs and visit notes), which took A LOT OF TIME, I learned today from the Perplexity Health AI: “So even though those note sets exist in your health system, what’s flowing into this connection right now is the coded summary, not the full written note body”.
To get Perplexity Health AI to review the visit note (not the summary, the actual note), I had to reupload the visit notes to the AI side of the conversation so it could read those vs. the coded summaries.
With that in mind, Guava’s AI had me copy the line from the visit note that I wanted it to compare with my other visit notes. This is what Guava Health’s AI told me today: “I can review excerpts you paste here, but I can’t directly pull provider notes from your chart unless the app exposes them to me in this chat. If you want, paste the relevant sections”.
The Patient’s Reality
Asking a hospital’s HIM department to fix a third-party AI’s mapping is an exercise in futility. We don’t have the energy to act as unpaid data engineers for a Beta product that is already charging a premium. Also, what do you think the hospital system would say if I asked for this?
Help Desk Emails
I have emailed the help desk for Perplexity Health AI and Guava. Because I did so about the above issue with Perplexity Health AI at the suggestion of the AI after it realized it was missing significant biomarker data points, let’s address the difference.
Perplexity Health: AI Support Agent Sam emailed me back to thank me for my insights and saying that they forwarded my feedback about lab integration limitations, file upload limits, and suggestions to the product team. I sent the email April 14, 2026. I haven’t heard back.
Guava Health: This is one example of an email with the Guava Help Desk. I emailed Guava Health’s Help Desk and asked how to fix an issue when there were two sources for the same lab on August 7, 2025. On August 8, 2025, I received an email from Alex Yau, Founder and President of Guava Health to answer my question. He asked for a screenshot for an example, which I sent and he followed up with additional insight and added that he would forward it to his team to give more thought.
Note. Both Perplexity Health AI and Guava Health have discords. I am not in the Perplexity discord, but I am in the Guava Health Discord.
The Android OS Barrier
While iOS users have a native Hub, Perplexity is “desktop-primary” for Android users. Using a mobile browser to check your health data is clunky and lacks the seamless utility of a native app.
The Repository Advantage: DICOM, Quest, and GI Notes
Guava is a Source of Truth; Perplexity is a search window.
- Imaging (DICOM): Guava supports actual X-ray, CT, and MRI image files. You aren’t just storing a “report”; you are carrying your entire imaging library in your pocket. (Note. You need to upload those, but, still.)
- Medication Reconciliation: I manage 62 active medications. Guava allows me to merge and deduplicate them across providers. Perplexity was able to retrieve some medication lists from the facilities BUT some of those lists were outdated.
My understanding is that Perplexity Health AI integrates with Apple Health for medication management, but I use Android, so I cannot comment on that.
I can, however, comment on Guava Health’s Medication management:
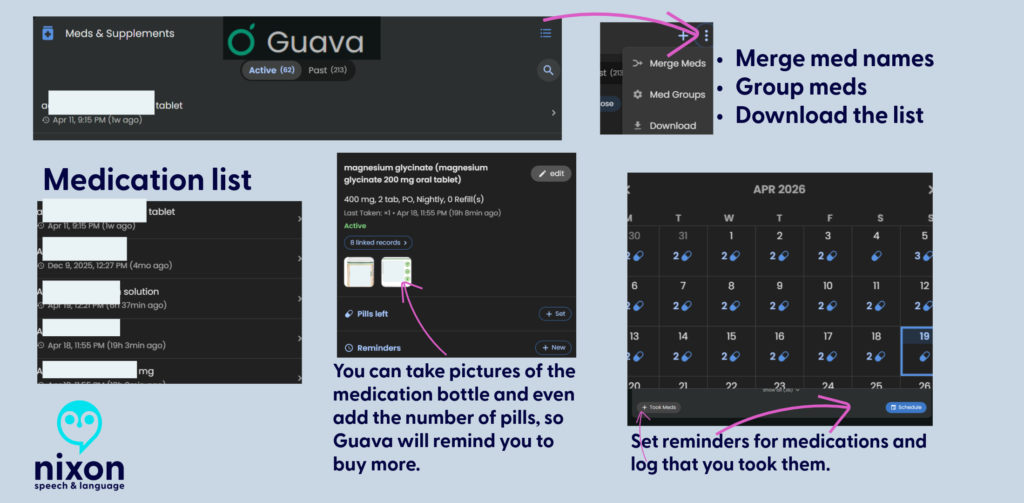
Data Portability: The “Disability & Tax” Hack
The true power of a health platform is what you can do with the data.
- The Guava Hack: I downloaded my encounter history from Guava and used Gemini (in thinking or data analysis mode) to generate a mileage CSV for my taxes and a total encounter count for other paperwork. Guava provided the “raw material” to simplify my legal and financial life.
- Perplexity’s Failure: Because Perplexity couldn’t accurately aggregate my history, I question whether it could do so accurately.
I’ll talk more about this in another post.
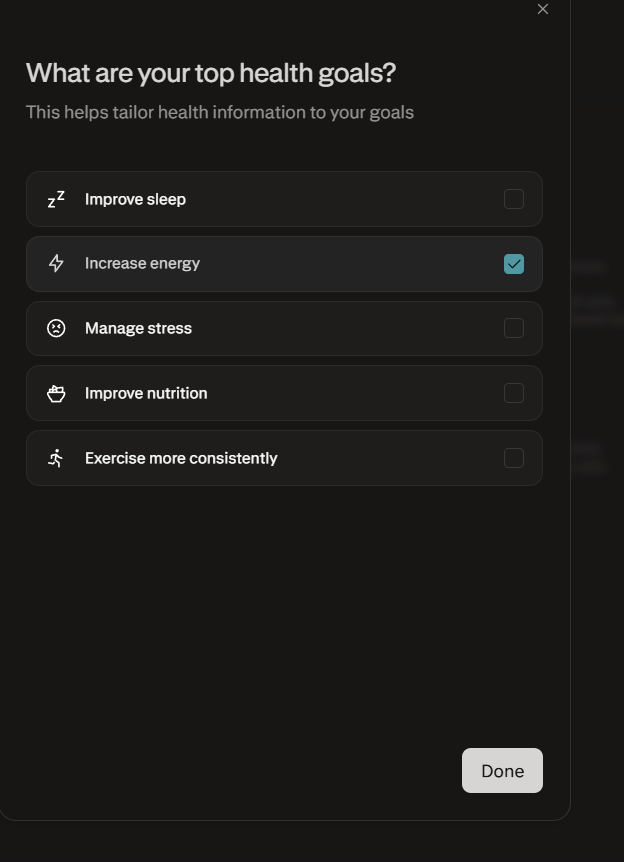
Setting Health Goals in Perplexity
One of the most revealing disconnects in Perplexity’s “Health Hub” is the Health Goals feature, which feels fundamentally “un-Spoonie.” While the marketing suggests a personalized experience, the available goals are largely aspirational wellness targets—like “Improving sleep” or “Marathon training”—that assume a linear, healthy baseline.
For a patient managing chronic illness, these rigid targets are often inappropriate or even demoralizing, as they ignore the daily fluctuations in energy and capacity that define the “Spoonie” experience. In contrast, the Fitbit Beta with Gemini feels significantly more approachable; instead of assigning a generic wellness category, it begins with a conversation about your specific challenges and health conditions. This “Coach” approach allows the AI to adjust its insights to your actual reality, rather than forcing you into a “fitness enthusiast” mold that your body simply isn’t in today.
Auditing for Bias & The Privacy Trap
I decided to test Guava Health and Perplexity AI today on auditing visit notes for biased language from a specific former provider.
- While Perplexity was helpful, I found that NotebookLM and Gemini were significantly better at finding subtle linguistic cues.
- Guava Health had me copy and paste the lines from the visit note into the AI for analysis against my record, but the AI then gave me an excellent plain language overview of bias in the portion I provided it.
CRITICAL PRIVACY WARNING: Unless you have a signed BAA (Business Associate Agreement)—like Guava—BE AWARE that uploading sensitive records to any non-HIPAA compliant AI (e.g., Gemini via personal Gmail, NotebookLM attached to personal Gmail, ChatGPT, or Perplexity without the Perplexity Health piece) is only as secure as your cloud data/passwords/and more.
Final Verdict: Research vs. Management
Perplexity Health is charging a premium ($20/month) for a Beta product that requires the patient to act as a manual data entry clerk. It is for people who want to research a disease.
Guava Health is for people who have to manage one. Guava Health Premium is only $8 per month. And if your provider has a Guava Health Provider Dashboard and invites you to it, IT IS free for you. Guava Health also offers a free version to patients.
- Use Perplexity if: You want a search engine for medical trends. (Maybe? But I still haven’t tested this out as much as I need to. I tend to use Google Scholar.)
- Use Guava if: You need to manage medications, prepare questions for medical visits, quickly access provider notes, see overviews of your biomarkers, store your imaging, and have your data work for you in the real world.
COMING SOON:
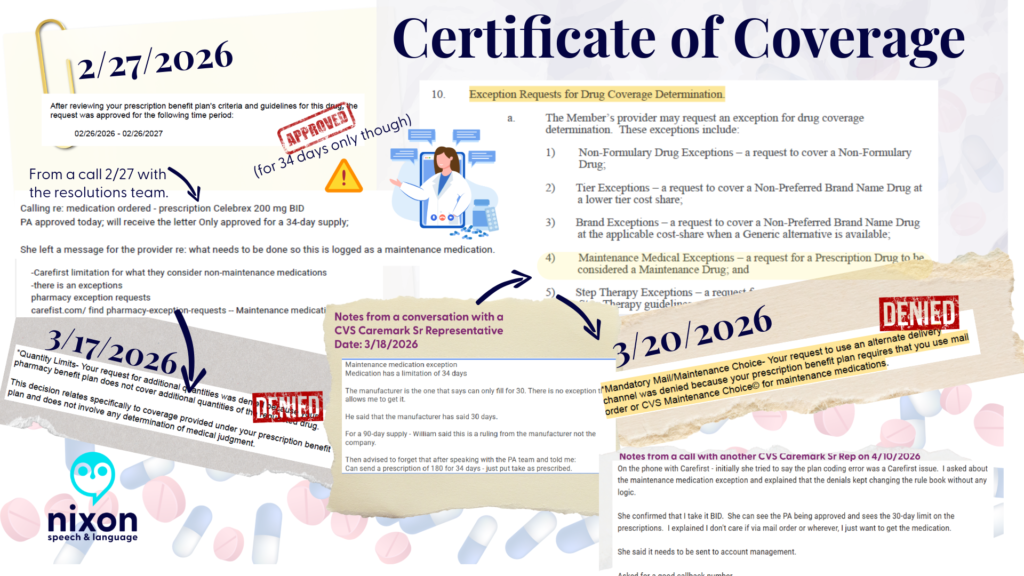
- How to get a copy of your evidence (certificate) of coverage
- The Disability & Tax Guide: A step-by-step on using your medical data to navigate these two data heavy tasks.
- The Provider Portal: How Guava helps your doctors help you.
- Guava Tags: How I use custom tagging to find patterns in flares.
If you have questions about Guava Health, post them here!
Visit the Platforms
Identification Note: Logos used for nominative fair use for critical review. Stephanie Nixon, PhD, CCC-SLP serves on the Guava Patient Advisory Panel pro bono. Review based on the April 2026 Beta of Perplexity Health.
chronic illness, Guava Health, Health apps, Perplexity Health AI, Spoonie life